Fig. 4.1
Abundant repeated hemoptysis, complications of an old bronchiectasis. (a) CT, parenchymal windows: bilateral basal severe bronchiectasis. (b) Mediastinal window, sagittal oblique reconstructions: voluminous BA arising from the aorta at T5 level; bilateral alveolar condensation. (c) Descending aorta angiography showing this BA. (d) Selective angiography (Mikaelsson catheter); frontal view: right–left common BA, hypervascularization of the left inferior lobe and of the right base. The CT/angio confrontation leads to decide a bilateral embolization. (e) Selective microcatheterization: bilateral distal particular embolization, authorizing the preservation of the arterial access, in order to later re-embolize if necessary

Fig. 4.2
Possible origins of ectopic BA (from aortic arch or descending aorta below T6) and possible origins of aberrant BA (from subclavian, internal thoracic A, thyro bicervical trunk, coronary A, etc.)
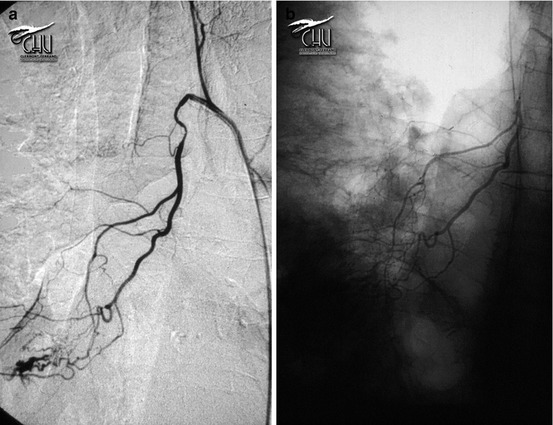
Fig. 4.3
Common right intercostobronchial trunk. (a) Semi-selective catheterization: hilar hypervascularization. (b) Hyperselective catheterization, downstream intercostal arteries, which warrant embolization without out-of-target occlusion (anterior radiculo-medullary artery arising from an intercostal artery)

Fig. 4.4
Abundant and repeated hemoptysis in a severely scoliotic old woman: CT has localized the bleeding coming from right superior lobe. (a) Aortogram: extremely sinuous thoracoabdominal aorta; large right BA. (b) Selective catheterization: common right + left BA trunk, with a right intercostobronchial trunk. This unstable catheterization led us to use absorbable gelatine sponge (Gelfoam) as occlusion agent. (c) Post-embo angiogram
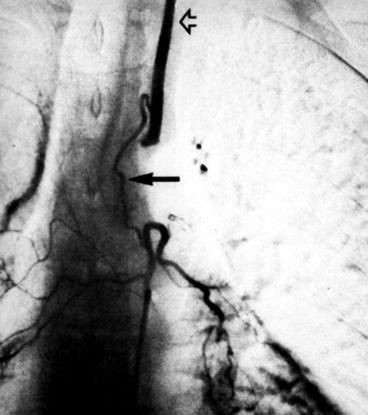
Fig. 4.5
Anastomosis between left BA and left vertebral A (arrow)
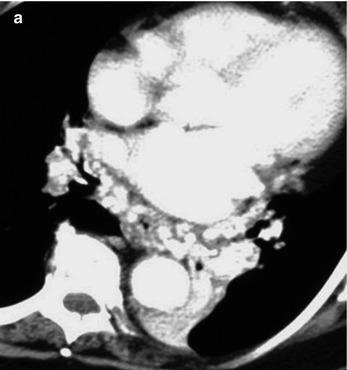
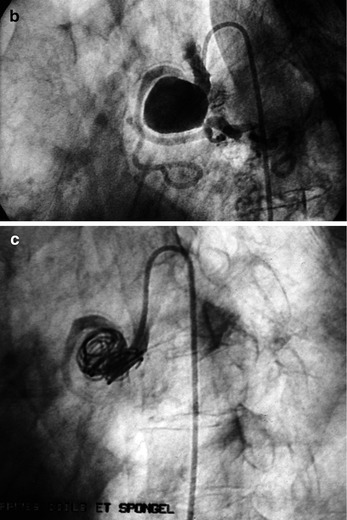
Fig. 4.6




Repeated abundant hemoptysis, complication of an old tuberculosis in an old patient. (a) Important systemic right bronchial hypervascularization; a right BA origin is suspected on lung CT analysis. (b) Right BA selective catheterization: voluminous proximal BA aneurysm. (c) Post-embo (coils + Gelfoam) angio control
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
