A 41-year-old woman, the mother of 3 offspring, with likely heterozygous familial hypercholesterolemia, had been asymptomatic until age 38 when angina pectoris and exertional dyspnea appeared leading to the discovery of severe multivessel coronary artery disease and a massively calcified ascending aorta. Coronary bypass grafting using the right and left internal mammary arteries did not alleviate the symptoms. Evidence of overt heart failure subsequently appeared and that led to heart transplantation at age 41. She died 22 days later. The occurrence of massive diffuse calcification of the ascending aorta and minimal focal calcification of the abdominal aorta is rare and in the patient described it appears to be the consequence of heterozygous familial hypercholesterolemia.
Heavy calcific deposits in the ascending aorta are infrequent. Patients with huge abdominal aortic aneurysms or huge calcific deposits in the wall of the abdominal aorta infrequently, for example, have significant calcific deposits in the ascending aorta. Patients with familial hypercholesterolemia, particularly the homozygous variety, typically have heavy calcific deposits in ascending aorta and few if any calcific deposits in abdominal aorta, the reverse of the usual situation. Patients with non-familial hypercholesterolemia typically have heavy calcific deposits in their abdominal aorta and few, if any, in the ascending aorta. We recently studied a 41-year-old woman who had huge diffuse calcific deposits in the ascending aorta and minimal focal deposits in the abdominal aorta, and evidence of familial hypercholesterolemia of the heterozygous variety. Patients with a “porcelain” aorta are infrequently considered to have familial hypercholesterolemia. A description of this occurrence in this setting is the purpose of this report.
Description of Patient
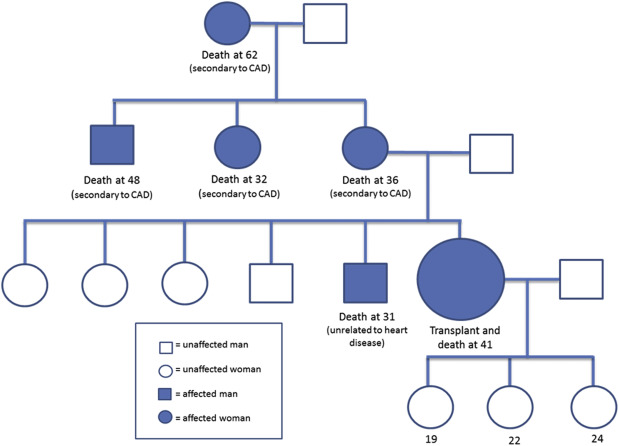
This 41-year-old white woman was born in January 1973 and died in December 2014. Her family tree is shown in Figure 1 . She underwent heart transplantation 22 days before death. (An autopsy was not performed.) A coronary artery bypass grafting procedure had been done in April 2012 because of angina pectoris and exertional dyspnea. Before that operation, coronary angiography had shown severe multivessel coronary disease ( Table 1 ). A stent had been inserted in the proximal right coronary artery. Heavy calcific deposits had been noted in the left main, left anterior descending, and left circumflex coronary arteries and in the ascending aorta. In November 2014, the patient was referred to Baylor University Medical Center. Computed tomography confirmed the massive calcific deposits in the ascending aorta and only a few focal deposits in the abdominal aorta ( Figure 2 ). Serum cholesterol and other values are shown in the table. She was on simvastatin 40 mg daily before these cholesterol values were evaluated. She had evidence of severe heart failure, a very low ejection fraction, and, global left ventricular hypokinesis.
| Angina pectoris | + |
| Dyspnea on exertion | + |
| Precordial murmur | + (grade3/6) |
| Diabetes mellitus (type II) | + |
| Systemic hypertension (by history) | + |
| Body mass index (Kg/m 2 ) | 26 |
| Mitral regurgitation | 2+/4+ |
| Aortic valve stenosis | 0 |
| Hematocrit (%) | 29 |
| Total cholesterol (mg/dl) | 135 |
| Low-density lipoprotein cholesterol (mg/dl) | 87 |
| High-density lipoprotein cholesterol (mg/dl) | 40 |
| Triglycerides (mg/dl) | 88 |
| Blood urea nitrogen (mg/dl) | 25 |
| Creatinine (mg/dl) | 1.2 |
| B-type natriuretic peptide (pg/ml) | 1970 |
| Magnesium (mg/dl) | 1.9 |
| Thyroid stimulating hormone (uIU/ml) | 0.95 |
| Creatinine clearance (ml/min) | 48 |
| Coronary artery narrowing (% diameter reduction): | |
| Right | 90%(ostial) |
| Left main | 10% |
| Left anterior decending | 99% |
| Left circumflex | 10% |
| Coronary bypass | + |
| Intracardiac defibrillator | + |
| Ejection fraction (%) | 25 |
| Pulmonary artery (mmHg) (s/d) | 35/26 |
| Pulmonary arterial wedge (mmHg) | a17 b17 m16 |
| Left ventricle (mmHg) (s/d) | 113/10 |
| Left ventricular angiogram | Global hypokinesis (severe) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


