of dislodgment of atherosclerotic debris or aortic dissection (Fig. 24.1). The so-called no-touch technique has evolved to better manage these patients (2). It relies on the internal mammary artery or gastroepiploic artery as conduits for coronary bypass grafts. In some patients requiring extensive revascularization, saphenous vein grafts can be anastomosed to the internal mammary artery. In no-touch cases, a femoral artery, axillary artery, or the underside of the distal aortic arch is used as the arterial cannulation site (2,3,4). Alternatively, either a long-arch cannula can be inserted distal to the left subclavian artery or a diffusion-tipped cannula can be used (5) to better disperse the flow jet at the CPB cannula tip. However, these cannulation techniques still present some risk of stroke hazard from insertion of the cannula in the severely diseased aorta. Cannulating from the left ventricular apex with the cannula advanced through the aortic valve has also been described (6).
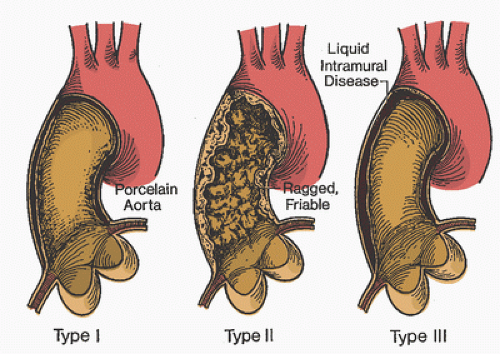 FIGURE 24.1. Type 1, type II, and type III ascending aortic atherosclerosis. No clamp is safe on these types of ascending aortic disease. Type I: Circumferential ascending aortic calcification, which may be easily diagnosed preoperatively on the angiogram. Palpation of the ascending aorta at operation reveals firm calcification. Embolization or aortic injury that may be difficult to repair may result if the aorta is clamped. Type II: This pattern may be diagnosed preoperatively by noting an irregularity of the normally smooth lining of the ascending aorta on the left ventricular angiogram or aortic root injection. Visualization of the ascending aorta is now considered a mandatory part of workup before coronary artery bypass graft. Type III: Intraluminal liquid debris is the most elusive of the three patterns to diagnose before clamping the aorta. A pale appearance of the aorta or adherence of the adventitia to the ascending aorta may be the only diagnostic clues. Operative echocardiography will reveal a thickened ascending aorta that will liberate liquid debris if a cross-clamp or partial occlusion clamp is applied. (From Mills NL, Everson CT. Atherosclerosis of the ascending aorta and coronary artery bypass: pathology, clinical correlates, and operative management. J Thorac Cardiovasc Surg 1991;102:546-553, with permission.) |
undergo hemolysis, which can be severe, depending largely on the thermal amplitude and titer of the cold agglutinin. For hemolysis to occur, the cold agglutinin and complement activities must overlap. That is, the temperature must be low enough for the cold agglutinins to activate but warm enough for a complement fixation to occur.
TABLE 24.1. Characteristics of cold agglutinins | ||||||||
|---|---|---|---|---|---|---|---|---|
| ||||||||
several weeks, by which time the antibody may have disappeared (17). If the urgency of surgery precludes that approach, the most sensible approach is to use either normothermia or mild hypothermia using blood temperatures continuously maintained above the thermal amplitude to avoid the active temperature range of agglutination (17,19,20,21,22,23). Hence, the presence of cryoagglutinins with high titer or high thermal amplitude may represent a reasonable indication for the use of warm cardioplegia myocardial protection techniques while maintaining normothermic systemic temperatures.
varies with the individual, but sickle cell disease patients typically have predominantly hemoglobin S. This homozygous state is found in 0.15% of African-Americans and is associated with severe hemolytic anemia and vaso-occlusive phenomena, resulting from the increased blood viscosity that occurs when red blood cells aggregate and individually typically assume a sickle shape (29). Sickled cells have a very limited capacity to load and unload oxygen.
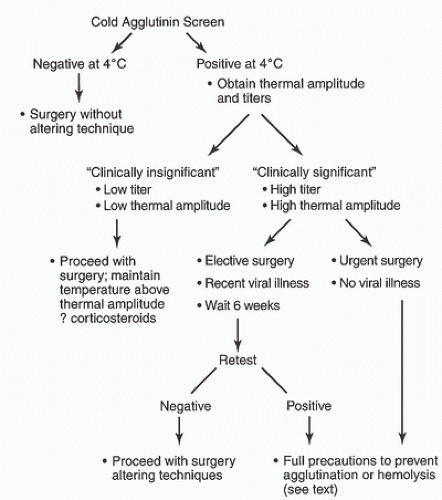 FIGURE 24.2. Algorithm for management of cold agglutinins in cardiopulmonary bypass. |
flows and avoiding low cardiac output states both before and after bypass.
faith it is mandatory because of their strict interpretation of the bible (63). More than 50 years ago, Cooley et al. (64) first reported the feasibility of open-heart surgery in this patient population. In 1977, Ott and Cooley (65) reported additional results in a large series of Jehovah’s Witness patients in whom no blood was transfused. However, there was a 10.7% mortality in those undergoing CPB (n = 39), with preoperative or postoperative anemia a contributing factor in 12 deaths.
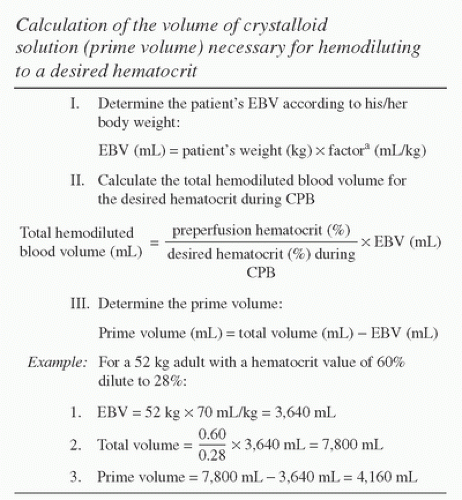 FIGURE 24.3. Calculation of volume of crystalloid solution (cardiopulmonary bypass prime volume) necessary for hemodiluting to a desired hematocrit. EBV, estimated blood volume; CPB, cardiopulmonary bypass. aFactor (EBV/kg) is assumed to be 80 mL/kg for <10 kg body weight; 75 mL/kg for 10 to 20 kg of body weight; 70 mL/kg for >20 kg of body weight. The example addresses the polycythemic adult, but this condition is more prevalent in cyanotic pediatric patients with smaller required CPB circuit prime volumes. (From Milam JD, Austin SF, Nihill MR, et al. Use of sufficient hemodilution to prevent coagulopathies following surgical correction of cyanotic heart disease. J Thorac Cardiovasc Surg 1985;89:623-629, with permission.) |
vacuum may be manifested by intermittent or staccato flow; in severe situations, the venous line may rhythmically jerk and relax as flow stops and is then reestablished with systemic venous return in the patient’s cavae or right atrium. Levels of hemolysis will also quickly rise if excessive vacuum is exerted in the venous line (82).
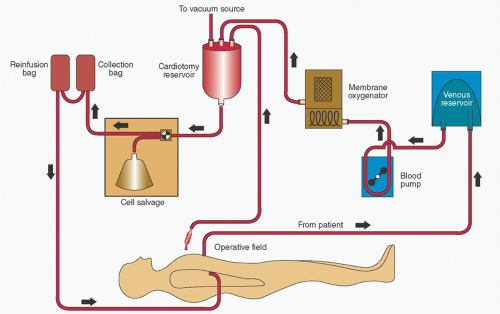 FIGURE 24.4. Schematic drawing of cardiopulmonary bypass (CPB) circuit for collection, processing, and reinfusion of blood after bypass while maintaining continuity with the patient’s circulation. The reinfusion bag (top left) should initially be back-filled with patient’s blood from an intravenous site to establish continuity with cell salvaged blood (from collection bag) before CPB. Cardiotomy suction can be used after bypass until protamine is administered with collected blood processed in the cell salvage system. Residual perfusate in the CPB circuit should be transferred to the cardiotomy reservoir and also processed by the cell-salvage system to minimize blood loss. A second cardiotomy reservoir (not shown) is used during CPB for conventional collection of suctioned and vent blood, which is drained into the venous reservoir. (Modified from Milan TP Jr, Whitmore J, Maddi R. Reoperative cardiac surgery in a Jehovah’s Witness: role of continuous cell salvage and in-line reinfusion. J Cardiothorac Anesth 1989;3:211-214, with permission.) |
blood). However, excessive hemodilution may predispose to pulmonary edema, which might be addressed by limiting hemodilution to a hematocrit fraction of more than 20% in postpneumonectomy patients.
TABLE 24.2. Perioperative measures to minimize blood loss in the Jehovah’s Witness patient | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
of the air and improve flow, the logic is flawed. Greater negative pressure will only serve to increase air entrainment and worsen the issues. The preferred approach would be to identify the source of the air entrainment and prevent further entrainment.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


