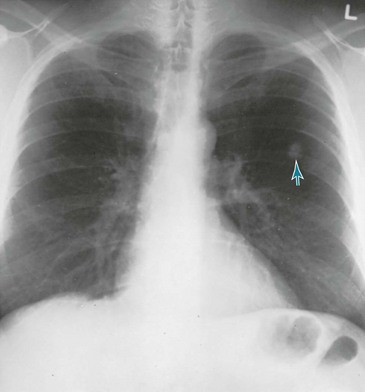
21 The goal of this chapter is to extend the discussion of lung cancer into the clinical realm and relate how the pathologic processes considered in Chapter 20 are encountered in a clinical setting. An outline of the major clinical features of lung cancer is followed by a discussion of the diagnostic approach and general principles of management. The chapter concludes with a brief discussion of bronchial carcinoid tumors, malignant mesothelioma, and the clinical problem of the solitary pulmonary nodule. Distant metastases, most commonly to the brain, bone or bone marrow, liver, and adrenal gland(s), frequently are asymptomatic. In other cases, symptoms depend on the particular organ system involved. Small cell carcinoma is the cell type most likely to generate distant metastases (see Chapter 20). Squamous cell carcinoma is least likely, and both adenocarcinoma and large cell carcinoma occupy an intermediate position. Other paraneoplastic syndromes cannot be attributed to a known hormone, and our understanding of their mechanisms varies. Examples range from a wide variety of neurologic syndromes (some of which appear to be due to autoimmune antibody production) to the soft tissue and bony manifestations of clubbing and hypertrophic osteoarthropathy (see Chapter 3). The nonspecific systemic effects of malignancy, such as anorexia, weight loss, and fatigue, are potential consequences of lung cancer, and it has been hypothesized that production of various mediators, such as tumor necrosis factor, may mediate these systemic effects. The initial test for detection and macroscopic evaluation of bronchogenic carcinoma is generally the chest radiograph. The presence of a nodule or mass within the lung on chest radiograph always raises the question of lung cancer, especially when the patient has a history of heavy smoking. The location of the lesion may give an indirect clue about its histology: peripheral lesions are more likely to be adenocarcinoma or large cell carcinoma, whereas central lesions are statistically more likely to be squamous cell carcinoma or small cell carcinoma (Figs. 21-1 and 21-2). The chest radiograph is also useful for determining the presence of additional suspicious lesions, such as a second primary tumor or metastatic spread from the original carcinoma. Involvement of hilar or mediastinal nodes or the pleura (with resulting pleural effusion) may be detected on the chest radiograph, and such a finding will substantially affect the overall approach to therapy. Figure 21-2 Chest radiograph shows adenocarcinoma of lung manifesting as solitary pulmonary nodule (arrow). A newer technique that has gained increasing popularity in the evaluation of patients with known or suspected lung cancer is positron emission tomography (PET; see Chapter 3). Because of their high metabolic activity, malignant lesions typically exhibit high uptake of the radiolabeled glucose analog 18F-fluorodeoxyglucose (FDG). Focal uptake in the region of a parenchymal nodule or mass suggests the lesion is malignant, and uptake in the mediastinum or at distant sites often reflects spread of the tumor to those sites. However, other metabolically active lesions (e.g., focal areas of infection) may also show FDG uptake, so a positive PET scan in the appropriate clinical scenario is very suggestive but is not diagnostic of malignancy. The best way to directly examine the airways of a patient with presumed or known bronchogenic carcinoma is by bronchoscopy with either a rigid or, much more frequently, a flexible bronchoscope (see Chapter 3). The location and intrabronchial extent of many tumors can be directly observed, and samples can be obtained from the lesion, either for cytologic or histopathologic examination. In addition, the bronchoscopist can assess whether an intrabronchial carcinoma is impinging significantly on the bronchial lumen and causing either partial or complete airway occlusion. Diagnostic specimens can be obtained in many cases even when the lesion is beyond direct visualization with the bronchoscope. In recent years, significant technologic advances in bronchoscopy, such as endobronchial ultrasound and electromagnetic navigation techniques, have increased the diagnostic yield of the procedure for lesions that are difficult to sample by direct visual or fluoroscopic guidance alone.
Lung Cancer
Clinical Aspects
Clinical Features
Symptoms Relating to Nodal and Distant Metastasis
Paraneoplastic Syndromes
Diagnostic Approach
Macroscopic Evaluation
Lung Cancer: Clinical Aspects




