Fig. 2.1
(a, b) SFJ anatomy
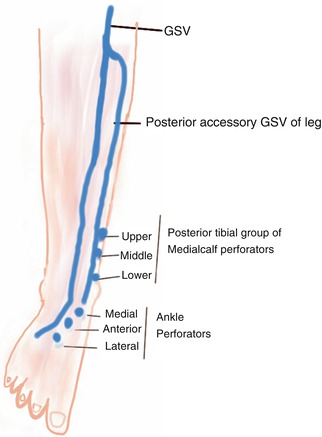
Fig 2.2
Posterior tibial group of medial calf perforators
The location of the SFJ as per textbooks of anatomy is 4 cm below and lateral to the pubic tubercle [5]. However, during surgery of high ligation, by intraoperative measurement we have localized it to a mean of 2.7 cm below and 3 cm lateral to the pubic tubercle. Any incision used to expose the SFJ should use the pubic tubercle as a landmark. Two valves are located at this point. About 1 cm proximal to the junction, a terminal valve can be found almost consistently. There is another preterminal valve about 3 cm distal to the first one [4]. These valves are bicuspid with the concave leaflets facing upward. Weight of blood coming backward onto the concavity of the leaflets fills them and causes them to fall backward. This prevents further flow and maintains the competence of the valve.
Tributaries of GSV [1]
(a)
Near termination: The confluence of superficial inguinal veins – formed by superficial circumflex iliac vein, superficial epigastric and external pudendal veins, and the distal GSV.
(b)
At the thigh: Anterior accessory and posterior accessory GSV of the thigh.
(c)
At the leg: Anterior accessory and posterior accessory GSV of the leg. The posterior accessory GSV of the leg was known as posterior arch vein or Leonardo’s vein.
The accessory veins lie at a slightly anterior plane compared to the GSV outside the saphenous compartment. At the saphenofemoral junction, there could be a variable number of other unnamed tributaries [7].
Saphenous Nerve and Its Relation to the GSV
Saphenous nerve is the largest branch of the femoral nerve and is a purely sensory nerve. It descends along with the femoral artery. It exits the adductor canal at its distal end, pierces the fascia lata, and becomes subcutaneous. In the lower part of the leg, it is in close proximity to the GSV. The nerve can be damaged during surgical stripping and endovenous procedures. The damage is less likely at the upper part of the leg because of the larger gap between the nerve and vein here.
Short Saphenous Vein (SSV)
The SSV originates from the lateral side of the foot and drains into the popliteal vein. The following anatomical facts are important in surgery of SSV:
(a)
The SSV pierces the deep fascia of the leg at the mid calf level and runs between the two heads of the gastrocnemius to enter the popliteal vein. The upper one-third of the SSV lies below the deep fascia [8, 9]. Hence, the deep fascia of the popliteal fossa has to be incised to expose the terminal portion of the SSV.
(b)
The termination of the SSV can be variable. Three types of terminations have been described – Kosinski’s variations [8, 9].
Normal termination (57 %) – enters the popliteal vein in the popliteal fossa
High termination (33 %) – ends in the mid thigh in a muscular vein or the GSV
Low termination (10 %) – ends in the deep veins of the calf or deep sural muscular veins or GSV in the upper third of the leg
(c)
The sural nerve courses along the SSV in the distal part of the calf. In a study on the fascial anatomy of SSV of 20 embalmed human specimens, it has been reported that the distance between the SSV and the sural nerve was less than 5 mm in proximal 1/3 of the lower leg in 70 % of specimens; the deep fascia was present between the SSV and the sural nerve in more than 95 %. In the distal 2/3 of lower leg, the distance between the SSV and the sural nerve was less than 5 mm in 90 % and the deep fascia was present between the two structures in only 15 %. Hence, the sural nerve is at risk of thermal injuries during endovenous thermal ablation in the lower leg [10].
(d)
The vein of Giacomini (intersaphenous vein) runs in the posterior part of the thigh and connects the SSV with the GSV. A SSV projection or tributary ascending in the thigh above 12 cm from the popliteal skin crease is designated as the Giacomini vein irrespective of the termination of the SSV (Fig. 7.6b). It is reported in 70.4 % of limbs. In the lower thigh, it is located below the deep fascia. In the middle and upper thigh, it perforates the deep fascia and ends in the superficial or deep veins or in the muscular veins. Its presence does not affect the position of SSV termination; nor does it affect the severity of venous disease [11, 12].
Deep Veins
More than 80 % of the blood flow in the lower limbs is through the deep veins. The deep veins of the lower extremity accompany the arteries and their branches. They possess numerous valves.
In the leg, these include the posterior tibial veins, anterior tibial veins, and peroneal veins. They are all paired structures. In the thigh, these include the popliteal vein, femoral vein, profunda vein, and the common femoral veins.
The pelvic veins include the external iliac, internal iliac, and common iliac veins and the inferior vena cava. The gonadal veins draining to IVC on right side and the renal vein on the left side are important vessels in the pathogenesis of pelvic congestion syndrome (PCS).
Perforating Veins [2, 6]
These veins perforate the muscular fascia to connect the superficial veins with the deep veins. Communicating veins connect veins within the same system [3]. There are as many as 150 perforating veins in the lower extremity, although only a few of these are clinically important [13, 14]. The medial calf perforators are probably the most important from the clinical point of view. Most perforators are inactive in the normal state. In the presence of venous hypertension, they open up and reflux blood to superficial veins.
Perforators in the foot: These consist of the dorsal, plantar, medial, and lateral perforators. Between the first and second metatarsal bones, a large perforating vein, connecting the superficial venous arch to the pedal vein, can be identified.
Perforators at the ankle: These are a cluster of vessels arranged as anterior, medial, and lateral groups.
Medial calf perforators: They are arranged in two groups:
(a)




Posterior tibial perforating veins: They were known as the Cockett perforators. They connect the posterior accessory GSV of the calf (posterior arch vein) with the posterior tibial vein. There are three of them: lower, middle, and upper, located just behind the medial malleolus and at 7–9 cm and 10–12 cm from the lower edge of the medial malleolus respectively. They are at 2–4 cm behind the medial edge of tibia. In perforator surgery, these are the vessels which are mainly targeted (Fig. 2.2).
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
