Low-Attenuation Mass, Mediastinum or Hilum
Jud W. Gurney, MD, FACR
DIFFERENTIAL DIAGNOSIS
Common
Diaphragmatic Hernia
Lipomatosis
Lipoma
Less Common
Low-Attenuation Lymph Nodes
Mediastinal Metastases
Infection: Fungal & Tuberculosis
Nerve Sheath Tumors
Mediastinal Abscess
Thymolipoma
Teratoma (Dermoid Cyst)
Mediastinal Cyst
Liposarcoma
Lymphangioma
Hemangioma
Thymic Cyst
Rare but Important
Mediastinal Pseudocyst
Lateral Meningocele
Epipericardial Fat Pad Necrosis
Extramedullary Hematopoiesis
Whipple Disease (Intestinal Lipodystrophy)
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Fat (-70 to -130 HU) vs. fluid (0-30 HU)
Mnemonic for fat-containing lesions: LITHE (yes, this is an oxymoron)
Lipomatosis, lipoma, liposarcoma
Intestinal lipodystrophy
Thymolipoma, teratoma (mature)
Hernias, hemangioma
Extramedullary hematopoiesis, epipericardial fat pad necrosis
Mnemonic for water density lesions: FLUIDS
Foregut duplication cysts, lymphangioma, pseudocyst, infection (nodes and abscess), desmoid, spine (meningocele)
Enlarged normal lymph nodes often have central fat or fatty hilum
Helpful Clues for Common Diagnoses
Diaphragmatic Hernia
Includes hiatal hernia, Bochdalek, Morgagni, and traumatic hernias
Contents typically include fat and bowel
Lipomatosis
Location: Upper mediastinum, costophrenic angles, paraspinal
Unencapsulated fat
Associated with generalized obesity, Cushing disease, corticosteroid therapy
Lipoma
Location: Typically anterior mediastinum
Encapsulated, may be pedunculated
Well-marginated, fat only
Any soft tissue component, consider liposarcoma or thymolipoma
Helpful Clues for Less Common Diagnoses
Low-Attenuation Lymph Nodes
Mediastinal Metastases
Metastases may be low attenuation from necrosis or cystic degeneration
Typical tumors include bronchogenic carcinoma, testicular, ovarian, and treated lymphoma
Infection: Fungal & Tuberculosis
Enlarged nodes with rim enhancement and low-attenuation centers
Indicates active disease
Nerve Sheath Tumors
Neurofibroma or schwannoma
Frequent low attenuation (15-20 HU) due to lipid content or cystic degeneration
Mediastinal Abscess
Descending cervical mediastinitis usually from odontogenic or cervicofacial infection, esophageal perforation, or trauma
Caudal spread aided by gravity and negative intrapleural pressure
Irregularly shaped fluid collections, may contain air
Thymolipoma
Anterior mediastinal mass, conforms to shape of adjacent structures
Typically large; mean length: 18 cm
Tumor contains mixture of fat (at least 50%) and soft tissue
Soft tissue seen as linear strands or whorls, uncommonly rounded nodules
Teratoma (Dermoid Cyst)
Anterior mediastinal mass
Fat in 75%, fluid in 90%
Mixture of fat, soft tissue, fluid, and calcification (50%)
Cystic component often predominant (multilocular), 15% cystic only
Mediastinal Cyst
Includes foregut duplication cysts, pericardial cysts
Cysts are thin walled, unilocular
Fluid attenuation variable: Water, hemorrhage, infection, milk of calcium
Bronchogenic cysts usually subcarinal; esophageal duplication cysts periesophageal; neurenteric cysts associated with adjacent vertebral body cleft
Liposarcoma
Location: Typically posterior mediastinum
Inhomogeneous with large areas of soft tissue density
Lymphangioma
Multilocular, well-defined, water density mass; may be septated
Location: Superior mediastinum adjacent to right lateral tracheal wall
Soft in composition, no mass effect
Intrathoracic lymphangiomas + cystic bone lesions = Gorham disease
Hemangioma
Location: Superior mediastinum
Fat in 40%, phleboliths in 10-40%
Thymic Cyst
Congenital cysts most common, usually unilocular
Acquired cysts usually multilocular
Occurs in patients after radiation therapy for Hodgkin disease, in association with thymic tumors, and after thoracotomy
Helpful Clues for Rare Diagnoses
Mediastinal Pseudocyst
Pancreatic pseudocyst extending through esophageal or aortic hiatus
Location: Posterior inferior mediastinum
Fluid collection, thin or thick walled
Usually connects to pancreatic pseudocysts
Lateral Meningocele
Associated with neurofibromatosis
May be multiple and bilateral
Typically enlarges neural foramen
Epipericardial Fat Pad Necrosis
Patients usually present with acute pleuritic chest pain
Imaging and pathologic features similar to those of fat necrosis in epiploic appendagitis
Extramedullary Hematopoiesis
Typically in patients with congenital hereditary anemias, especially thalassemia
Posterior mediastinal masses usually caudal to 6th thoracic vertebra
May contain fat, especially larger lesions
Centered on vertebral body with prominent trabeculae from marrow expansion
Whipple Disease (Intestinal Lipodystrophy)
Infection caused by Tropheryma whippelii
Migratory polyarthritis followed by intestinal malabsorption
Low-density nodes from foamy lipid-containing macrophages
Image Gallery
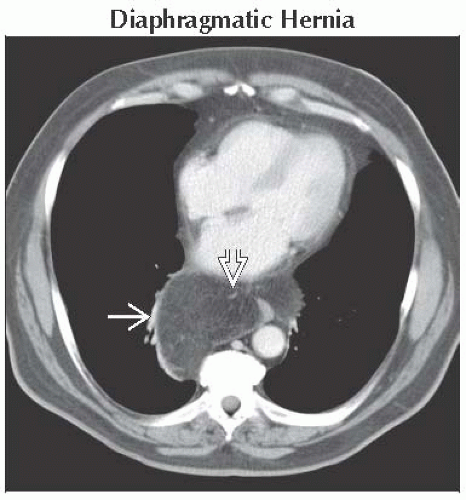 Axial CECT shows a hiatal hernia of peritoneal fat tissue through esophageal hiatus  . Note the sparse linear vessels . Note the sparse linear vessels  typical for herniated abdominal fat. typical for herniated abdominal fat. |
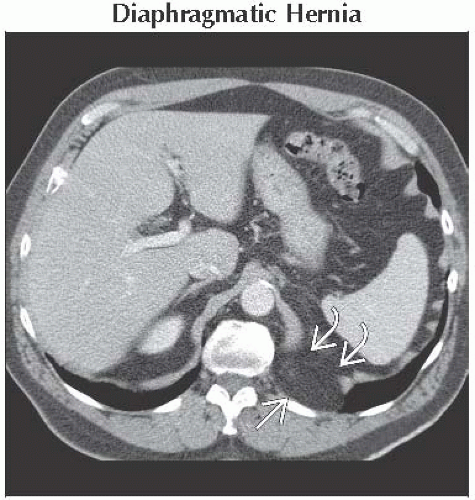 Axial CECT shows Bochdalek hernia containing retroperitoneal fat  . Note the localized discontinuity of the medial left hemidiaphragm . Note the localized discontinuity of the medial left hemidiaphragm  . . |
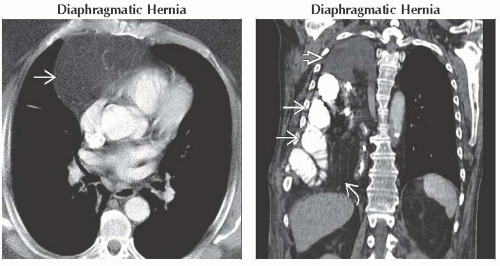 (Left) Axial CECT shows herniation of peritoneal fat
 through Morgagni hiatus. Morgagni hernias are typically right-sided; the left side is blocked by the heart. (Right) Coronal CECT shows large right pleural effusion through Morgagni hiatus. Morgagni hernias are typically right-sided; the left side is blocked by the heart. (Right) Coronal CECT shows large right pleural effusion  , small bowel loops , small bowel loops  , and peritoneal fat , and peritoneal fat  from traumatic diaphragmatic tear. Right-sided tears are less common than tears of the left hemidiaphragm. Coronal reconstructions are often useful for diaphragmatic hernias. from traumatic diaphragmatic tear. Right-sided tears are less common than tears of the left hemidiaphragm. Coronal reconstructions are often useful for diaphragmatic hernias.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|