Level 1
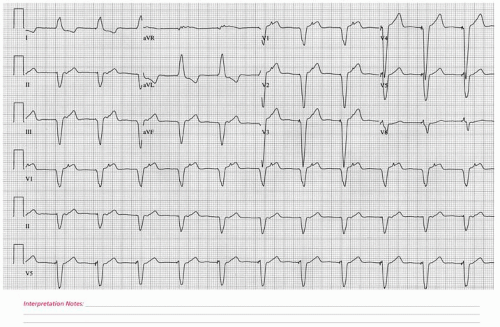
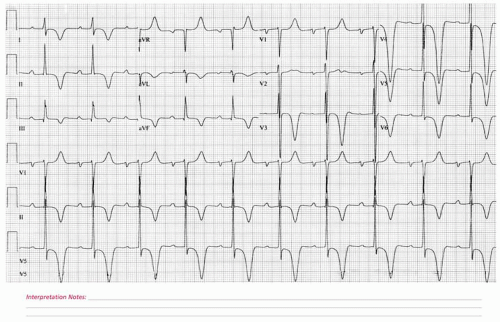
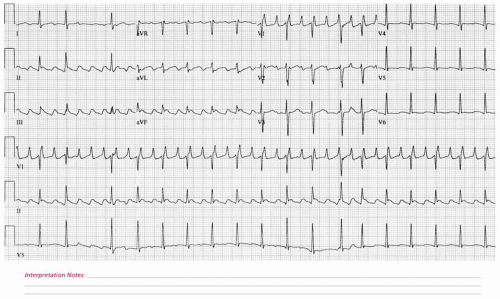
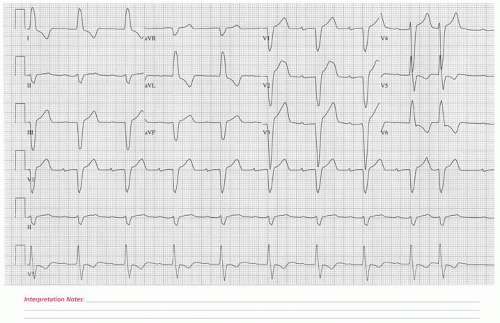
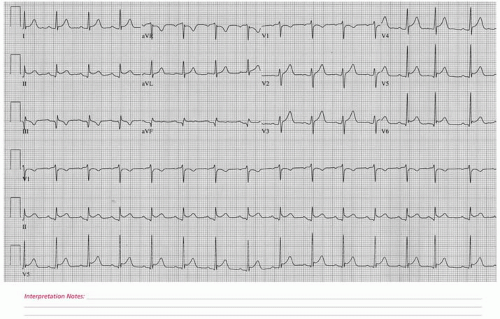
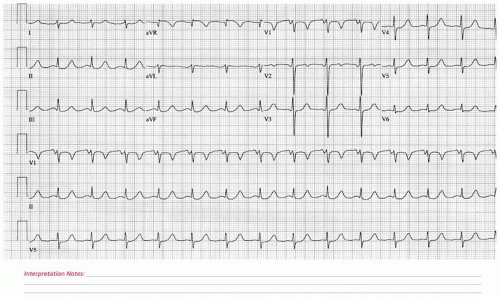 ECG 1 A 60-year-old female with severe coronary artery disease and severe aortic stenosis who underwent successful multi-vessel coronary artery bypass grafting and bioprosthetic aortic valve replacement. This electrocardiogram was obtained on the first postoperative day in the cardiothoracic surgery intensive care unit. |
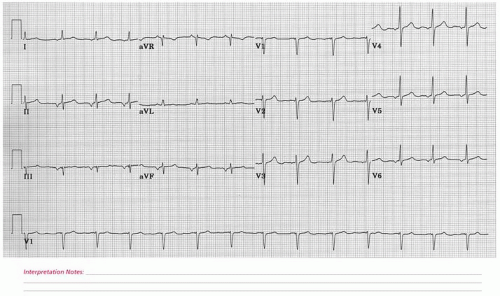
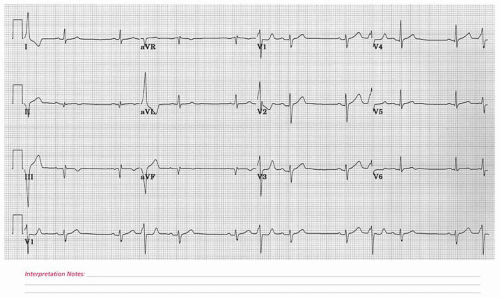
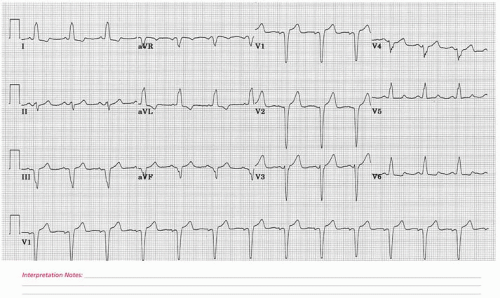
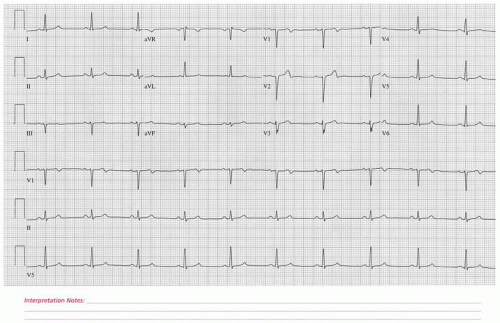
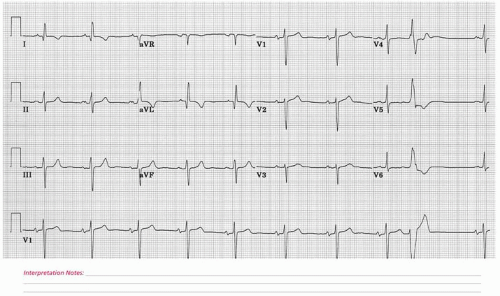
 ECG 2 A 34-year-old male with congenital bicuspid aortic valve disease and severe aortic valve insufficiency. |
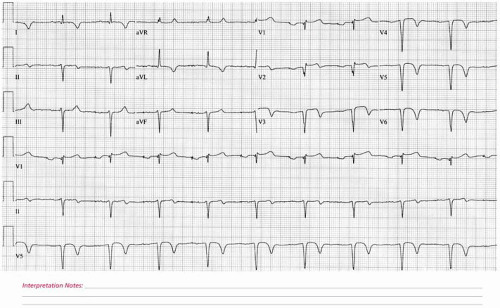
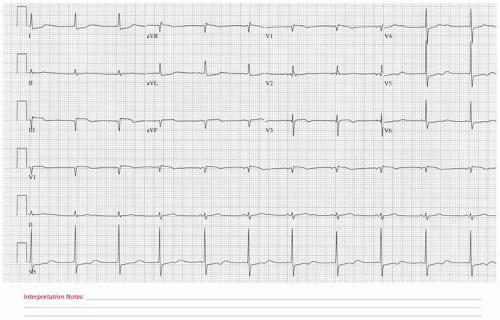
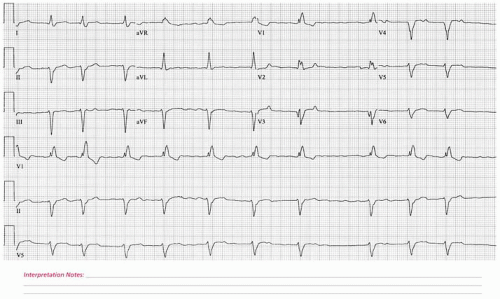
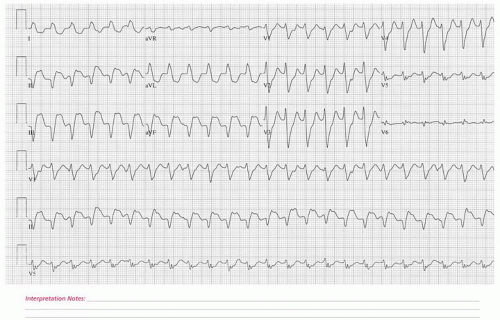
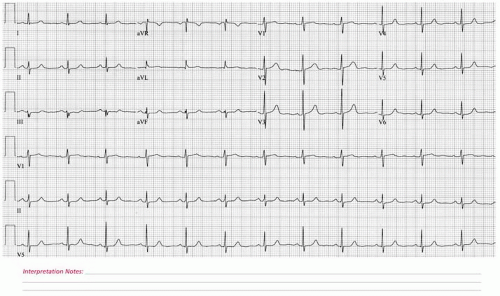
 ECG 3 A 54-year-old female with a history of metastatic malignant melanoma who is being evaluated for a subsequent course of chemotherapy. Her past cardiac history includes an angioplasty to the left circumflex coronary artery 8 years prior to this tracing. She is currently asymptomatic. Her cardiac medications included diltiazem and aspirin. |
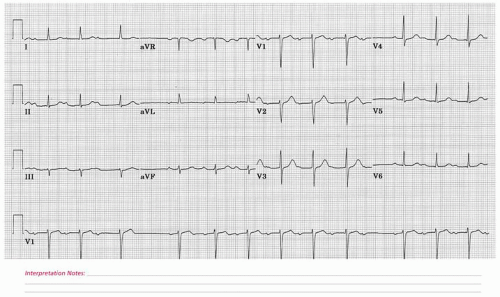
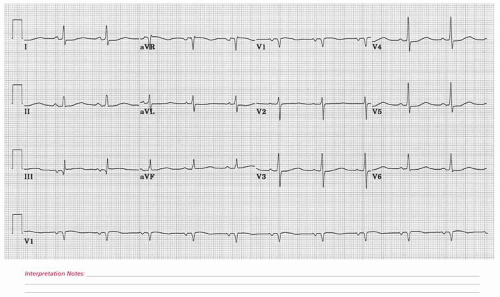
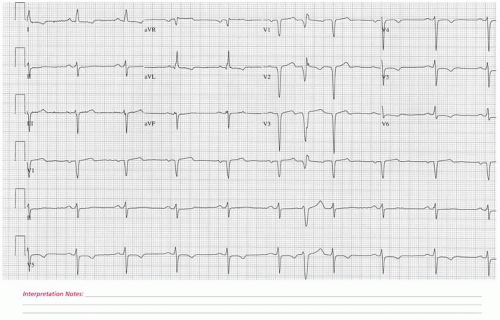
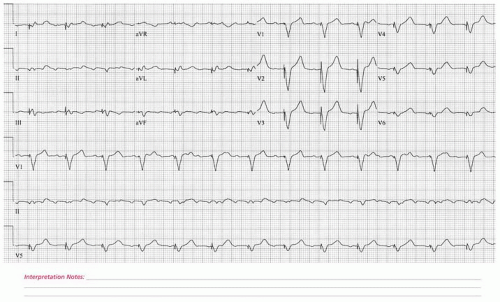
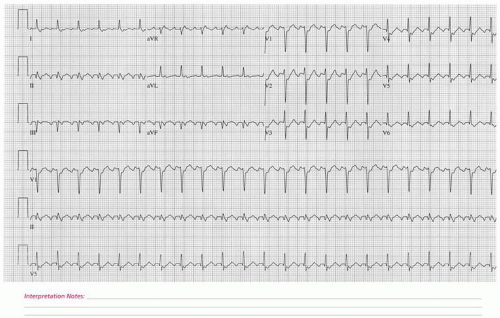
 ECG 4 An 82-year-old male with known ischemic heart disease who suffered a large myocardial infarction 2 years prior to this electrocardiogram. His myocardial infarction was complicated by transient decompensated congestive heart failure and persistent bradycardia, necessitating placement of a permanent pacemaker. He now returns for outpatient cardiovascular medicine follow-up, feeling well with the exception of mild dyspnea upon exertion. |
 ECG 5 A 78-year-old male with recent symptoms of lightheadedness and one episode of syncope. |
 ECG 6 A 70-year-old female who presents for a general physical examination. She has a history of coronary artery obstructive disease and is status post a myocardial infarction of unknown location 4 years prior to this electrocardiogram. Other comorbid conditions include extensive past tobacco use, hypertension, and gastroesophageal reflux disease. Her medications at the time of this electrocardiogram included potassium, thyroxine, triamterene/hydrochlorothiazide, and Naprosyn. |
 ECG 7 A 67-year-old female with a history of paroxysmal atrial fibrillation and long-standing hypertension who returns for an outpatient cardiac electrophysiology follow-up evaluation. She feels well at the present time with excellent perceived control of her atrial fibrillation. Two years prior to this electrocardiogram, a left heart catheterization was performed, demonstrating normal coronary arteries. |
 ECG 8 A 74-year-old female with recent pacemaker placement and postprocedure persistent shortness of breath. |
 ECG 9 A 52-year-old male with coronary artery disease who presented to the hospital with an accelerating pattern of angina pectoris. Comorbid conditions include hyperlipidemia, hypertension, peptic ulcer disease, and chronic anxiety. Medications at the time of this electrocardiogram included aspirin, simvastatin, cholestyramine, a multivitamin, metoprolol, and topical nitroglycerin. |
 ECG 10 A 70-year-old male recently diagnosed with lung cancer now seen in the oncology outpatient department. He has a history of long-standing hypertension, hyperlipidemia, and advanced coronary artery disease, for which he underwent a multi-vessel coronary artery bypass grafting operation approximately 1 year before this electrocardiogram was obtained. |
 ECG 11 A 66-year-old male with known coronary artery disease and a prior coronary artery bypass operation. He has been experiencing 2 hours of severe chest pain and hypotension. |
 ECG 12 A 40-year-old male with renal failure secondary to chronic pyelonephritis awaiting renal transplant. His calcium level at the time of this electrocardiogram was greater than 11 mg/dL. |
 ECG 13 A 34-year-old female with a 2-week history of sudden-onset and progressive shortness of breath seen as a new patient in the outpatient department. She gave birth to her first child 2 weeks previously, concluding an uneventful pregnancy. Decompensated congestive heart failure was suspected. She was admitted to the hospital with transthoracic echocardiography demonstrating a left ventricular ejection fraction of 20% and moderately severe mitral regurgitation. |
 ECG 14 A 68-year-old male with long-standing hypertension and known coronary artery disease. |
 ECG 15 A 72-year-old male with advanced peripheral vascular disease who is admitted to the hospital for a semielective below-the-knee amputation. His past medical history includes chronic obstructive pulmonary disease, a remote myocardial infarction, and prior pacemaker placement. |
 ECG 16 A 47-year-old male who presented acutely to his local emergency room in the setting of sudden-onset severe anterior chest tightness with shortness of breath and profound fatigue. The patient was transported by helicopter to a facility with a cardiac catheterization laboratory at which time urgent coronary angiography and percutaneous coronary artery revascularization transpired. |
 ECG 17 A 67-year-old male with acute-onset chest pain of 2-hour duration. |
 ECG 18 A 79-year-old female with a history of non-insulin-requiring diabetes mellitus who was referred to the emergency room from her private physician’s office in the setting of acute-onset bilateral shoulder discomfort, shortness of breath, and nausea. A cardiac catheterization was performed 4 days after her hospitalization and demonstrated advanced disease in the right coronary artery, which was successfully treated with percutaneous transluminal coronary angioplasty. Medications at the time of this electrocardiogram included aspirin, metoprolol, glyburide, intravenous nitroglycerin, and intravenous heparin. |
 ECG 19 A 60-year-old male with intermittent shortness of breath referred for a cardiovascular medicine evaluation in the context of his symptoms and abnormal 12-lead electrocardiogram. The patient has otherwise remained well with a normal functional capacity and no known history of hypertension with frequent blood pressure checks over the years. |
 ECG 20 A 42-year-old male with known coronary artery disease and a myocardial infarction 2 years previously at which time urgent stenting of his left circumflex coronary artery was successfully undertaken. |
 ECG 21 A 79-year-old female with known coronary artery disease and moderately severe left ventricular systolic dysfunction who was re-referred for cardiac evaluation secondary to increasing angina pectoris. Medications at the time of this electrocardiogram included furosemide, metoprolol, Premarin, and aspirin. |
 ECG 22 An 83-year-old male who returns for cardiovascular medicine follow-up after suffering an acute myocardial infarction 2 months prior to this visit. With the exception of fatigue, he feels well and has resumed most of his daily activities without restriction. A transthoracic echocardiogram demonstrated a left ventricular ejection fraction of 35% with a regional wall motion abnormality confined to the infarction zone. No significant valvular heart disease was seen. |
 ECG 23 A 68-year-old male with a history of coronary artery disease who experienced a myocardial infarction 3 years previously. The patient returns for outpatient cardiovascular medicine follow-up. |
 ECG 24 A 46-year-old male with a myocardial infarction 2 years before this electrocardiogram who presented to the emergency room with a 6-hour history of acute severe substernal chest discomfort. The patient underwent emergent cardiac catheterization and percutaneous transluminal coronary angioplasty of a severe proximal left anterior descending coronary artery stenosis. |
 ECG 25 A 71-year-old male with long-standing hypertension, atrial fibrillation and mitral regurgitation who presented acutely to the emergency room with sudden-onset palpitations, lightheadedness, and profound fatigue. On presentation, the patient was found to be confused and hypotensive, undergoing semi-urgent direct current cardioversion. Two days later, he re-presented with recurrent heart palpitations but otherwise was less symptomatic with the accompanying electrocardiogram obtained at that time. |
 ECG 26 A 78-year-old female who presented 24 hours earlier with severe anterior chest discomfort consistent with an acute myocardial infarction. |
 ECG 27 A 56-year-old male with severe left ventricular systolic dysfunction in the setting of normal coronary arteries who is awaiting cardiac transplantation. His medications included thyroxine, furosemide, hydralazine, isosorbide dinitrate, captopril, and amiodarone. |
 ECG 28 A 68-year-old male with a recently experienced reversible ischemic neurologic event who was found on post-event evaluation to possess a severe obstruction of his right internal carotid artery. This electrocardiogram was obtained on the first postoperative day following a successful carotid endarterectomy. |
 ECG 29 A 41-year-old male with an acute myocardial infarction and cardiogenic shock. |
 ECG 30 A 61-year-old male with coronary artery disease and ischemic left ventricular systolic dysfunction who presents urgently to the hospital with an acute chest discomfort syndrome. His medications included potassium, isosorbide mononitrate, furosemide, glyburide, lisinopril, and warfarin. |
 ECG 31 A 44-year-old male who has experienced recent-onset shortness of breath and exertional lightheadedness. He subsequently consulted with his primary care physician, who auscultated a heart murmur and obtained this 12-lead electrocardiogram. A cardiovascular medicine consultation was arranged, and soon thereafter both an exercise echocardiogram and cardiac magnetic resonance imaging were performed. He underwent successful open-heart surgery. |
 ECG 32 A 62-year-old female admitted to the hospital with suspected unstable angina. She has no known coronary artery disease. |
 ECG 33 A 47-year-old male who presented to an outside medical facility with an electrocardiogram consistent with an acute inferior myocardial infarction. He received urgent thrombolytic therapy and was accepted in hospital transfer for cardiac catheterization. Comorbid conditions included long-term tobacco use and hypercholesterolemia. A cardiac catheterization demonstrated severe right coronary artery disease, which was treated with percutaneous transluminal coronary angioplasty and a intravenous thrombolytic infusion. |
 ECG 34 A 71-year-old male with a long-standing heart murmur who was diagnosed with severe bicuspid aortic valve stenosis. The patient underwent successful bioprosthetic aortic valve replacement. Postoperatively he suffered from recurrent atrial dysrhythmias and complete heart block, for which a permanent pacemaker was implanted. This electrocardiogram was obtained 2 weeks after his open-heart surgery. His chief concern was unremitting fatigue. |
 ECG 35 A 48-year-old female seen in the preoperative clinic prior to anticipated right knee surgery. The patient has no known cardiac history and with the exception of her knee abnormality maintains an excellent level of health. |
 ECG 36 A 66-year-old female who was scheduled for an elective stress test at which time the above electrocardiogram was obtained. She was admitted to the hospital to exclude acute myocardial injury. Acute myocardial injury was excluded, and subsequent stress testing suggested myocardial ischemia. A cardiac catheterization was performed demonstrating normal left ventricular systolic function and normal coronary arteries. |
 ECG 37 A 29-year-old male with recent-onset anterior chest pain, worse with deep inspiration who was seen in an urgent walk-in clinic. As part of his evaluation, a 12-lead electrocardiogram was performed. This was deemed abnormal, and he was referred to see a cardiologist. His chest discomfort has since resolved, and it was suspected to be musculoskeletal in origin. |
 ECG 38 A 78-year-old female with long-standing poorly controlled hypertension and nonischemic left ventricular systolic dysfunction. |
 ECG 39 A 45-year-old male who presented to an outside emergency room with a one-half-hour history of acute chest discomfort radiating to both shoulders and hands. The patient underwent urgent cardiac catheterization, which demonstrated a 100% proximal right coronary artery occlusion with superimposed thrombus. The patient underwent successful percutaneous transluminal coronary angioplasty. Cardiac enzymes were positive for acute myocardial injury. |
 ECG 40 A 74-year-old female who returns for an outpatient cardiac electrophysiology follow-up evaluation in the context of past permanent pacemaker placement. Two years prior to this appointment, the patient was experiencing periods of presyncope and fatigue. Holter monitoring demonstrated normal sinus rhythm, no significant dysrhythmias, and periods of intermittent heart block. Since her pacemaker was placed, her symptoms have resolved, and she reports returning to her normal activity level without impediment. |
 ECG 41 A 78-year-old female with intermittent lightheadedness and near fainting who presented to the emergency room with profound fatigue. |
 ECG 42 A 43-year-old male admitted in urgent hospital transfer after a 1-day history of acute chest discomfort. The patient was taken urgently to the cardiac catheterization laboratory where a 90% mid-left anterior descending coronary artery stenosis involving a second diagonal branch was present. The patient underwent successful angioplasty and stent deployment. |
 ECG 43 A 20-year-old female without a known health history who is seeing her primary care physician for her annual college sports physical exam. She feels well at the present time and is devoid of cardiac symptoms. She is a competitive college athlete and has demonstrated consistent performance improvement. |
 ECG 44 A 79-year-old male with recurrent syncope, status post recent permanent pacemaker implantation. |
 ECG 45 A 65-year-old male status post an inferior myocardial infarction 14 years previously. He subsequently underwent coronary artery bypass graft surgery and is currently asymptomatic. The above electrocardiogram was performed as part of his routine follow-up evaluation. |
 ECG 46 An 87-year-old male who returns for a primary care evaluation and follow-up examination. He feels well at the present time with the exception of intermittent fatigue and joint pain attributable to his osteoarthritis. He has a history of hypertension, hypertensive heart disease manifest by left ventricular hypertrophy on transthoracic echocardiography, and chronic obstructive pulmonary disease. |
 ECG 47 An 86-year-old male with fatigue, shortness of breath, and lightheadedness who was admitted to the coronary intensive care unit. Shortly after this electrocardiogram was obtained, a ventricular pacemaker was implanted. |
 ECG 48 A 65-year-old male referred for coronary artery bypass graft surgery in the setting of pulmonary edema and advanced coronary artery disease. A recent cardiac catheterization demonstrated moderately severe left ventricular systolic dysfunction and anterolateral akinesis. The most advanced coronary artery obstruction was in the diagonal branch of the left anterior descending coronary artery. Medications at the time of this electrocardiogram included atenolol, aspirin, simvastatin, and isosorbide mononitrate. Comorbidities included hypertension and long-term tobacco use. |
 ECG 49 An 84-year-old female who is seeing her primary care physician for her annual check-up. She feels well. She has a history of hypertension, well controlled on daily medication. She voices no concerns at this time and is able to walk 1-mile distance daily without stopping. |
 ECG 50 A 66-year-old male with known coronary artery disease who is acutely admitted to the hospital after presenting to the emergency room with a 10-hour history of incessant rapid heartbeating, shortness of breath, and chest tightness. |
 ECG 51 A 66-year-old male with a several-hour history of acute anterior chest discomfort who received urgent intravenous thrombolytic therapy. This electrocardiogram was obtained several hours after thrombolytic administration. The patient subsequently underwent cardiac catheterization, which demonstrated moderate diffuse coronary artery disease with the exception of a large second diagonal branch of the left anterior descending coronary artery, which was 100% occluded with superimposed thrombus. |
 ECG 52 A 67-year-old female who recently underwent a comprehensive physical examination. As part of her evaluation, she underwent a 12-lead electrocardiogram. This was abnormal prompting a cardiovascular medicine consultation. She feels well at the present time. Her past history includes hyperlipidemia, hypertension, and glaucoma. |
 ECG 53 A 42-year-old male with a known ostium secundum atrial septal defect, status post repair 2 years prior to this electrocardiogram who returns for cardiovascular medicine outpatient follow-up evaluation. |
 ECG 54 A 37-year-old male admitted to the coronary intensive care unit with syncope in the setting of advanced sinus bradycardia. The patient subsequently underwent permanent pacemaker implantation. |
 ECG 55 A 67-year-old female with a recent acute myocardial infarction who underwent a left heart catheterization demonstrating severe coronary artery disease. She promptly underwent coronary artery bypass grafting surgery. This 12-lead electrocardiogram was obtained on the 2nd postoperative day. |
 ECG 56 A 50-year-old male with known coronary artery disease and a prior myocardial infarction who is postoperative day 1 following coronary artery bypass grafting surgery. |
 ECG 57 A 65-year-old male with a nonischemic dilated cardiomyopathy and moderately severe left ventricular systolic dysfunction who returns for cardiology follow-up in the setting of non-sustained ventricular tachycardia. His medications included aspirin, enalapril, and atenolol. A prior cardiac catheterization demonstrated mild coronary artery disease. |
 ECG 58 A 72-year-old female with a history of thyrotoxicosis complicated by atrial dysrhythmias seen in cardiovascular medicine outpatient follow-up. She was recently hospitalized for a transesophageal echocardiogram-guided cardioversion that was successful in restoring normal sinus rhythm. Unfortunately, shortly thereafter, her atrial dysrhythmia recurred. She is now seen to discuss her near-future management options.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|