Left Ventricular Hypertrophy and Failure
Allen P. Burke, M.D.
Joseph J. Maleszewski, M.D.
Left Ventricular Hypertrophy
Physiology and Causes
Cardiac hypertrophy is an adaptive response to an increased load (pressure or volume) on the ventricle (Table 143.1). It is integral to processes that govern both normal physiology (e.g., athletic hypertrophy) and abnormal pathology (e.g., heart failure). Ventricular hypertrophy is often secondary to conditions that result in increased afterload or tension experienced by the ventricular wall during systole. Left ventricular wall thickness inversely correlates with afterload, which is directly proportional to chamber diameter and chamber pressure (Laplace law). Left ventricular hypertrophy also causes decreased preload, or diastolic stretching that allows filling of the ventricle. Optimal ventricular filling increases stroke volume by the Frank-Starling law, allowing for compensated left ventricular function at early stages in conditions with increased preload.
A chronic volume load and high cardiac output result in compensatory left ventricular hypertrophy, similar to conditions causing increased afterload. Aortic and mitral insufficiency and left-to-right shunts cause increased ventricular volume and subsequent cardiac enlargement. Increased volumes associated with pregnancy will transiently cause an increase in ventricular size and mass that normalizes in the months after delivery.1
A chronic increase in afterload, such as systemic hypertension and aortic stenosis, results in concentric left ventricular hypertrophy (with an increase in ratio between wall thickness and internal radius), which is the result of increased numbers of sarcomeres with normal length, arrayed in parallel. Initially, the left ventricular chamber cavity is small. With persistent increases in afterload, compensatory ventricular hypertrophy can no longer occur, and progression to ventricular dilatation and heart failure ensues.
Nonconcentric (eccentric) left ventricular hypertrophy is a clinical and radiologic term indicating increased left ventricular mass with a normal ratio between relative wall thickness and internal cavity dimension (Fig. 143.1). Nonconcentric hypertrophy is theoretically the result of increased sarcomeres arranged in series, pathologically resembles a dilated ventricle with a thick wall, and is associated with conditions associated with volume overload and decompensated concentric left ventricular hypertrophy. It is important to note that the clinical term “concentric left ventricular hypertrophy” corresponds to the pathologic term, whereas “eccentric left ventricular hypertrophy” is not typically used in a pathologic context and should not be confused with “asymmetric hypertrophy” caused by predominant thickening of the septum. Moreover, the term eccentric is somewhat of a misnomer in that the hypertrophy is not “off-center” as the term would imply. “Eccentric left
ventricular hypertrophy” is typically described as “cardiac hypertrophy with dilatation” in autopsy specimens, although the radiologic definition depends not on chamber diameter by itself but ratio of wall thickness to cavity dimensions.
ventricular hypertrophy” is typically described as “cardiac hypertrophy with dilatation” in autopsy specimens, although the radiologic definition depends not on chamber diameter by itself but ratio of wall thickness to cavity dimensions.
TABLE 143.1 Causes of Left Ventricular Hypertrophy | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
In addition to increased ventricular load, there are a variety of conditions that result in hypertrophy. These include infiltrative diseases such as amyloidosis and cardiomyopathies. Cardiac hypertrophy of obesity and end-stage renal disease is often multifactorial and may involve hypertension and myocardial fibrosis. Ischemic heart disease has often been associated with left ventricular hypertrophy, also likely due to ischemic fibrosis, often with concomitant hypertension.2
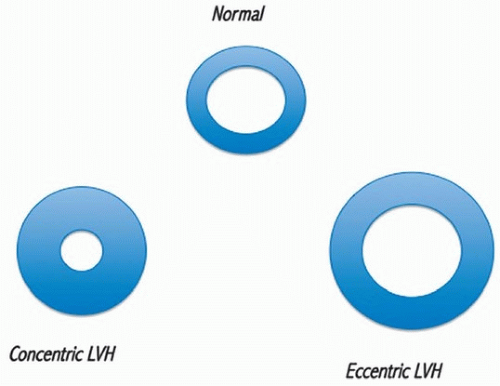 FIGURE 143.1 ▲ Concentric and eccentric left ventricular hypertrophy. By imaging, there is increased free wall thickness to cavity diameter ratio in concentric but not eccentric left ventricular hypertrophy, because of chamber diameter increase in the latter. |
“Asymmetric left ventricular hypertrophy” denotes increased left ventricular mass predominantly caused by septal hypertrophy. It is typical of hypertrophic obstructive cardiomyopathy and is seen in a minority of patients with hypertensive cardiomyopathy, aortic stenosis, and cardiac amyloidosis.
The concept of “idiopathic left ventricular hypertrophy” has been applied to patients with echocardiographic concentric left ventricular hypertrophy in the absence of other conditions that could explain it (ischemic, valvular, and hypertensive forms of heart disease).3 Often used in series of sudden death, the term is linked often with athlete’s heart.4 For autopsy diagnosis, in which case a history of hypertension is not always available or there is not other end organ damage (e.g., hypertensive nephropathy), the term “idiopathic left ventricular hypertrophy” can be used as a cause of death or descriptive term, when there are no anatomic or histologic abnormalities reflecting underlying cardiac disease.
In order to get an idea about the factors governing left ventricular hypertrophy in an autopsy specimen, it is critical to evaluate ventricular thickness and left chamber diameter excluding trabeculae and papillary muscles, at the level of the papillary muscles (see Chapter 1). The ventricular septal thickness needs to be measured separately, for evaluation of asymmetry (normally, the VS:FW < 1.3).
Epidemiology
In a series of elderly American men with high cardiovascular risk, 83% of whom had systemic hypertension, 66% had left ventricular hypertrophy by transthoracic echocardiography, 22% severe.5 In a relatively younger Han Chinese population, the prevalence of left ventricular hypertrophy was 43%, about evenly split between concentric and eccentric types.6 In autopsy series of sudden cardiac death, left ventricular hypertrophy is a very common finding, present in over 80% of hearts.7 Black race may be a risk factor for cardiomegaly in hypertension.7,8
Radiologic Findings
Echocardiographic assessment of left ventricular hypertrophy is more sensitive than electrocardiography, when corrected for body weight9,10. Currently, the radiologic gold standard for assessing left ventricular hypertrophy is magnetic resonance imaging, which can evaluate fibrosis.11 Cardiac magnetic resonance imaging has been used to define subsets of hypertrophy, with dilated and nondilated forms of both eccentric and concentric hypertrophy.12
Gross Findings
In the absence of significant right ventricular hypertrophy, heart weight, as adjusted to body weight or body size, is the ultimate gold standard of the degree of hypertrophy. Heart weight must be evaluated in context of sex and body size, and there are several resources available for this adjustment.13,14 Although it has been proposed that 383 g is the upper limit of normal for a man’s heart,15 this assessment was based on young men with a mean age of 23 and is therefore not useful for older individuals, as it is established that heart weight increases with age.16 An estimation of cardiomegaly based on a ratio to body weight or body surface area (heart weight index) is often used in animal studies (using body weight) and occasionally in human autopsy studies (using body surface area as estimated by the square root of the height). By the latter formula, a normal heart weight index is 200 mg/m2.17 However, a more practical approach is by defining cardiomegaly as a heart that weighs >50% above the expected mean (based on the individual’s size or weight).
Performing parallel short-axis sections from midventricle to the apex allows for good visual assessment of left ventricular hypertrophy. Traditionally, left ventricular wall thickness ≥15 mm is indicative of hypertrophy, but one must be aware that cardiac rigor (increased thickness) and decomposition (decreased thickness, so-called agonal dilatation) may affect the measurements. Care should be taken to avoid measuring recesses formed by trabeculations or papillary
muscles. In patients with hypertension, there is frequent coexistent right ventricular hypertrophy.8 The degree of chamber dilatation is important to record, primarily for determination of the presence of pressure (Figs. 143.2 and 143.3) or volume hypertrophy (Figs. 143.4, 143.5, 143.6).
muscles. In patients with hypertension, there is frequent coexistent right ventricular hypertrophy.8 The degree of chamber dilatation is important to record, primarily for determination of the presence of pressure (Figs. 143.2 and 143.3) or volume hypertrophy (Figs. 143.4, 143.5, 143.6).
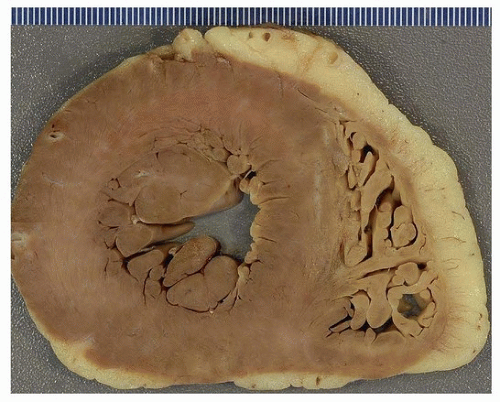 FIGURE 143.2 ▲ Concentric left ventricular hypertrophy. There is concentric thickening of the left ventricular wall, with a normal cavity diameter. The patient had hypertension and a 550-gram heart. |
Microscopic Findings
Left ventricular hypertrophy, in the pathologic sense, is a form of cardiac remodeling that consists of myocyte hypertrophy and perivascular-and pericellular-type interstitial fibrosis (Figs 143.7, 143.8, 143.9). There may be medial thickening of intramyocardial coronary arteries.18 Morphometric measurements of left ventricular samples taken from failing hearts demonstrate increased myocyte and nuclear size, increased interstitial collagen, and decreased microvascular density and microvascular lumen area.19,20 The number of binucleated myocytes does not appear to increase significantly.21
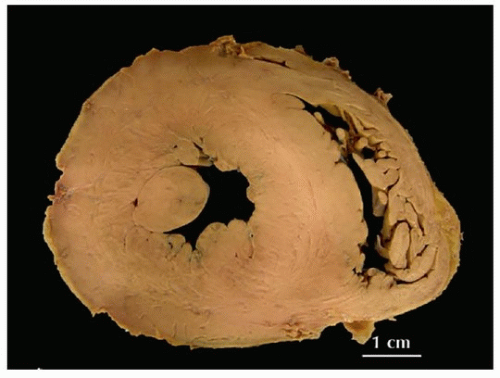 FIGURE 143.3 ▲ Concentric left ventricular hypertrophy. The appearance is similar to that shown in Figure 143.2. The patient had a severely stenotic (tricuspid) aortic valve with calcification (not shown). |
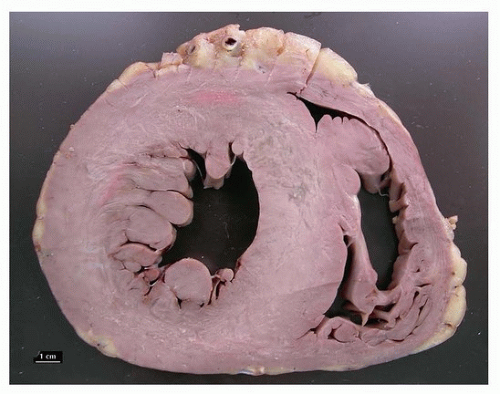 FIGURE 143.4 ▲ Concentric left ventricular hypertrophy with mild dilatation. The patient died suddenly and had marked concentric left ventricular hypertrophy (700 g) with mild chamber dilatation (4.5 cm). The patient had no history of hypertension, but renal vascular changes were highly suggestive of hypertensive renal disease. |
Endomyocardial Biopsy in Left Ventricular Hypertrophy
Native heart biopsy is generally performed in patients with unexplained heart failure, or to exclude cardiac amyloidosis. In patients with a clinical and imaging diagnosis of concentric left ventricular hypertrophy, the histologic changes are generally nonspecific, with amyloidosis confirmed in a small proportion. In about 5% of patients, lysosomeassociated membrane protein 2 mutations have been found, indicating a diagnosis of Danon cardiomyopathy.22 In about 1% of patients, Fabry disease will be confirmed based on alpha-galactosidase A activity and mutation analysis of the GLA gene.23
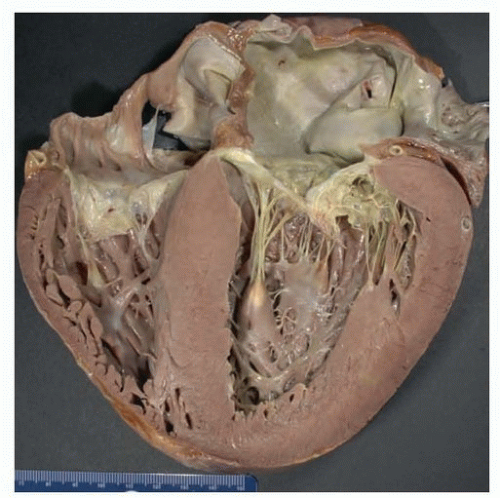 FIGURE 143.5 ▲ Concentric left ventricular hypertrophy with moderate dilatation. The heart weighed 600 g, and there was concentric thickening of the left ventricular wall (16 mm) with mild dilatation of the ventricular cavity (42 mm). The patient had long-standing hypertension and end-stage renal disease. |
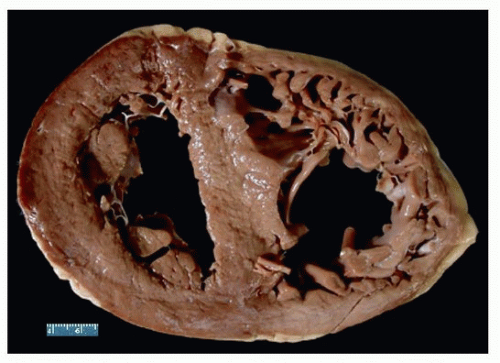 FIGURE 143.6 ▲ Cardiomegaly with biventricular dilatation. The heart weighed 750 g, in a morbidly obese patient who died suddenly after minor surgery. |
Prognosis and Outcome
Left ventricular hypertrophy leads to an increased risk of ventricular arrhythmias and sudden death, especially if there is concomitant heart failure. The risk factor-adjusted hazard ratio for sudden death ranged from 1.5 to 2.2 in echocardiography-documented left ventricular hypertrophy, which was highly significant.24 As assessed by two-dimensional echocardiography, increased left ventricular mass demonstrated a significant risk for cardiovascular death at 2 years, ranging from two to four times that of patients with normal-sized ventricles, depending on the severity of hypertrophy.25 The persistence and development of left ventricular hypertrophy as assessed by electrocardiography are associated with an increased risk of atrial fibrillation, the mechanism of which may be mediated by left atrial enlargement.26 Concentric left ventricular hypertrophy is an independent risk factor for both cardiovascular and all-cause mortality after heart transplant.27
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


