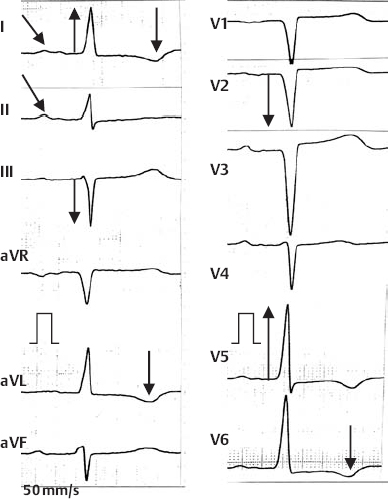
5.1 Left Ventricular Hypertrophy Left Ventricular Hypertrophy Mechanism: Hypertrophy of the left ventricular musculature as a consequence of systolic or diastolic overload This determines: Rotation of the cardiac axis in the superior and posterior direction Increase in voltage Lengthening of impulse conduction Relative ischemia of the inner layer with disturbed repolarization resulting in current flow from the outer to the inner layer ECG characteristics: Left axis to marked left axis deviation Widened QRS complexes (QRS up to 0.11 s; turning point in V5/6 > 0.05 s) High voltage of the R/S amplitudes (see indices) Left ventricular repolarization changes (T wave inversion, ST depression) Other criteria with left bundle branch block! Left Ventricular Hypertrophy Indices with left ventricular hypertrophy: Sokolow index (S V1 + RV5 > 3.5 mV) Sensitivity 25-43%, specifity 95% Lewis-Index (RI + S III – RIII-S I > 1,7 mV) Cornell-Index (RaVL + S V3 > 35 mm) Romhilt-Estes point system with assessment of: •Amplitude (Ror S in EA > 2.0 mV SV1-3 ≥ 2.5 mV, RV4-6 ≥ 2.5 mV) 3 points •Cardiac axis (left axis greater than -30°) 2 points •ST-T changes 1–3 points •QRS width (> 0.09 s, turning pointV5/6 > 0.05 s) 1 point each •Left atrial dilatation (P mitrale) 3 points → 5 points or more = criteria for left-ventricular hypertrophy •Sensitivity: 50-55%; specificity 95-98% Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: The Isthmus Region Acute Coronary Syndrome Resting Ischemia in the Anterior Wall Region Following Posterior Wall Infarction Medication-Related ECG Changes Stay updated, free articles. Join our Telegram channel Join Tags: Easy ECG Aug 29, 2016 | Posted by admin in CARDIOLOGY | Comments Off on Left Ventricular Hypertrophy Full access? Get Clinical Tree
5.1 Left Ventricular Hypertrophy Left Ventricular Hypertrophy Mechanism: Hypertrophy of the left ventricular musculature as a consequence of systolic or diastolic overload This determines: Rotation of the cardiac axis in the superior and posterior direction Increase in voltage Lengthening of impulse conduction Relative ischemia of the inner layer with disturbed repolarization resulting in current flow from the outer to the inner layer ECG characteristics: Left axis to marked left axis deviation Widened QRS complexes (QRS up to 0.11 s; turning point in V5/6 > 0.05 s) High voltage of the R/S amplitudes (see indices) Left ventricular repolarization changes (T wave inversion, ST depression) Other criteria with left bundle branch block! Left Ventricular Hypertrophy Indices with left ventricular hypertrophy: Sokolow index (S V1 + RV5 > 3.5 mV) Sensitivity 25-43%, specifity 95% Lewis-Index (RI + S III – RIII-S I > 1,7 mV) Cornell-Index (RaVL + S V3 > 35 mm) Romhilt-Estes point system with assessment of: •Amplitude (Ror S in EA > 2.0 mV SV1-3 ≥ 2.5 mV, RV4-6 ≥ 2.5 mV) 3 points •Cardiac axis (left axis greater than -30°) 2 points •ST-T changes 1–3 points •QRS width (> 0.09 s, turning pointV5/6 > 0.05 s) 1 point each •Left atrial dilatation (P mitrale) 3 points → 5 points or more = criteria for left-ventricular hypertrophy •Sensitivity: 50-55%; specificity 95-98% Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: The Isthmus Region Acute Coronary Syndrome Resting Ischemia in the Anterior Wall Region Following Posterior Wall Infarction Medication-Related ECG Changes Stay updated, free articles. Join our Telegram channel Join