Left-Sided Hemiparesis
A 31-year-old woman presented with sudden onset of left-sided hemiparesis. A cardiogenic embolic stroke was suspected and transthoracic echocardiography was performed; Video 9-1 and Figure 9-1 show a transthoracic echo — apical four-chamber view. A transesophageal echo was performed — Videos 9-2 and 9-3 and Figures 9-2 and 9-3.
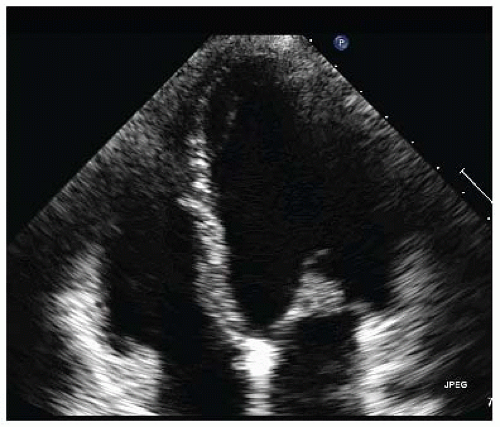 Figure 9-1. Transthoracic echocardiography shows a 0.7 × 0.7 cm mobile mass attached to the anterior mitral leaflet. |
QUESTION 1. How would you proceed to confirm a diagnosis?
A. Perform laboratory tests
B. Perform a transesophageal echocardiogram
C. Perform a magnetic resonance imaging
D. Start anticoagulation therapy immediately
E. Send the patient to surgery
View Answer
ANSWER 1: A. Laboratarory data should be collected to exclude infective endocarditis or malignant diseases causing nonbacterial thrombotic endocarditis. A systemic lupus erythematosus should be excluded as well (Libman-Sacks endocarditis).
Anticoagulation therapy is an option to prevent possible recurrent embolism due to superimposed thrombus formation attached to the cardiac mass.
A TEE should be performed to differentiate among intracardiac tumors, particularly among CPF, myxoma, and vegetation of endocarditis.
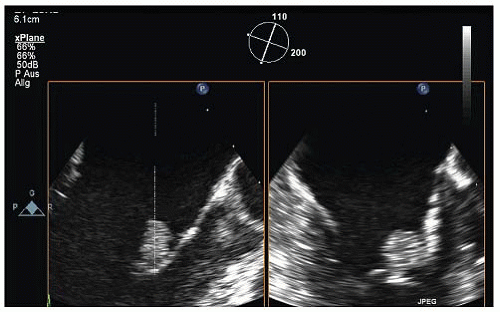 Figure 9-2. |
 Figure 9-3. 3D transesophageal echocardiogram (TEE) full volume. Enface view of the mitral valve—the mass is attached to the A1 segment of the anterior leaflet. |
QUESTION 2. The structure attached to the A1 segment of the anterior leaflet of the mitral valve is most likely:
A. An organized mobile thrombus
B. Nonbacterial thrombotic endocarditis
C. A pedunculated myxoma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


