Fig. 16.1
Folding Leaflet-plasty: (a) A 4-0 polypropylene suture is passed from the annulus, behind the elongated leaflet, emerging through the coapting edge. The needle then is passed back through the edge returning through the annulus. (b) The suture is then adjusted to reduce the leaflet edge is the same height as adjacent segments. Generally, this adjustment is guided by the saline filling test
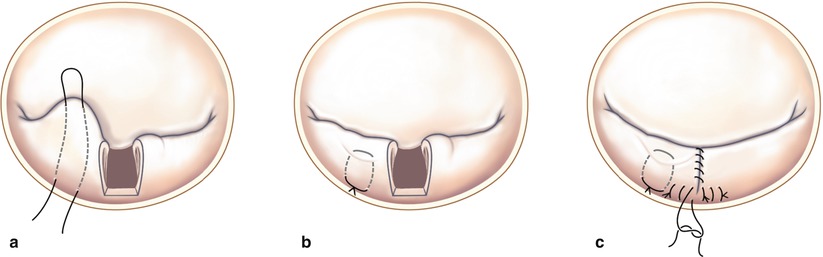
Fig. 16.2
(a–c) Picture of prolapsed mitral valve with quadrangular resection foldoplasty and resuturing of P2
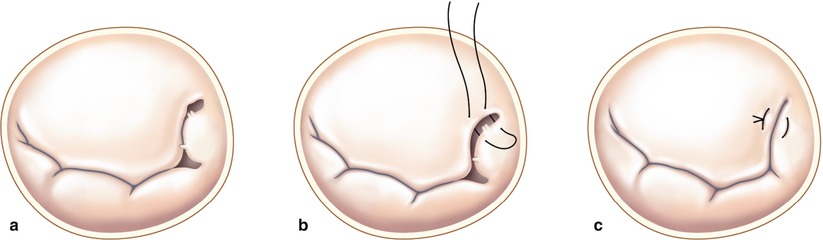
Fig. 16.3
Folding Leaflet-plasty combined with a Quadrangular Resection: In the presence of several prolapsing and elongated posterior leaflet scallops, several repair techniques can be combined. (a) A very large redundant P2 scallop has undergone a quadrangular resection. In parallel a P1 scallop folding-plasty is being started to reduce a slightly elongated prolapsing edge. An adjacent P2 quadrangular resection has been completed. (b) The P1 folding-plasty has been completed to reduce the leaflet height. (c) The quadrangular defect is then closed using a sliding-plasty along the annulus. Once P1 and P3 tissue have been advanced the residual defect is suture closed. In the end all posterior leaflet scallops should be of equal height
Tips and Pitfalls
The advantages of the folding valvuloplasty include technical simplicity and broad applicability, especially when performed robotically. Additionally, this technique allows a surgeon to undo and adjust the height of leaflet with minimal effort. Occasionally, we have found poor coaptation from an overly shortened posterior leaflet. This is corrected by removing and re-inserting folding plasty sutures after the annuloplasty ring is inserted.
Although a folding valvuloplasty can be used for any segment of posterior leaflet prolapse, we avoid this technique in patients with ruptured chords or flail leaflets. The folding leaflet-plasty should be avoided in the presence of papillary muscle rupture or a flail leaflet. It is feasible to combine a quadrangular resection and leaflet folding-plasty when multiple pathologies include a flail leaflet and a prolapsed posterior leaflet. In this situation a quadrangular resection can be performed, followed by a leaflet folding-plasty. Moreover, a leaflet folding-plasty can be performed after a quadrangular resection if P1 or P3 remains redundant following approximation of the remnant leaflet. Commissuroplasty is another simple technique not requiring leaflet resection (Fig. 16.3).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


