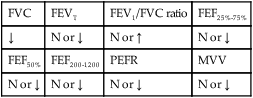
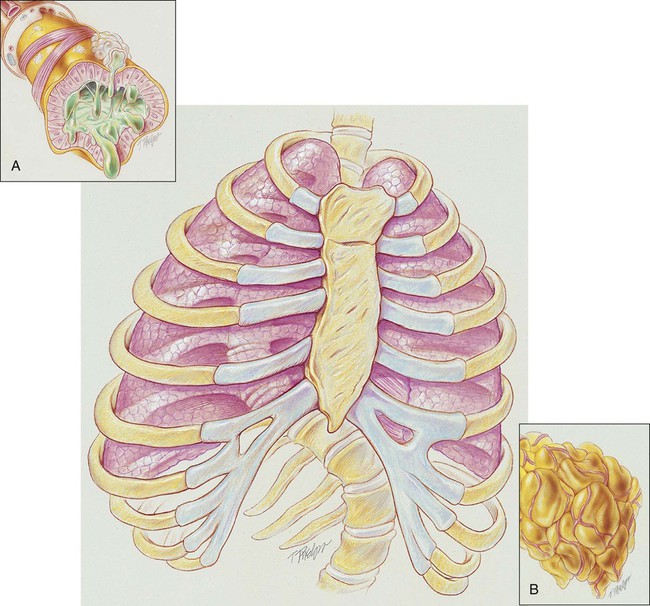
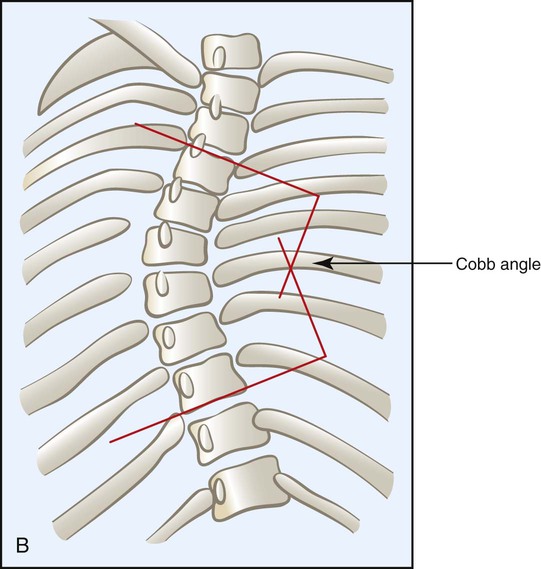
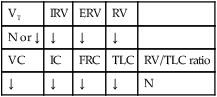
After reading this chapter, you will be able to: • List the anatomic alterations of the lungs associated with kyphoscoliosis. • Describe the causes of kyphoscoliosis. • List the cardiopulmonary clinical manifestations associated with kyphoscoliosis. • Describe the general management of kyphoscoliosis. • Describe the clinical strategies and rationales of the SOAPs presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. In severe kyphoscoliosis the deformity of the thorax compresses the lungs and restricts alveolar expansion, which in turn causes alveolar hypoventilation and atelectasis. In addition, the patient’s ability to cough and mobilize secretions also may be impaired, further causing atelectasis as secretions accumulate throughout the tracheobronchial tree. Because kyphoscoliosis involves both a posterior and a lateral curvature of the spine, the thoracic contents generally twist in such a way as to cause a mediastinal shift in the same direction as the lateral curvature of the spine. Severe kyphoscoliosis causes a chronic restrictive lung disorder that makes it more difficult to clear airway secretions. Figure 24-1 illustrates the lung and chest wall abnormalities in a typical case of kyphoscoliosis. • A condition caused by poor muscle control, muscle weakness, or paralysis because of diseases such as cerebral palsy, muscular dystrophy, spina bifida, or poliomyelitis. • Sex—Girls are more likely to develop curvature of the spine than boys. • Age—The younger the child is when the diagnosis is first made, the greater the chance of curve progression. • Angle of the curve—The greater the curvature of the spine, the greater the risk that the curve progression will worsen. • Location—Curves in the middle to lower spine are less likely to progress than those in the upper spine. • Height—Taller people have a greater chance of curve progression. • Spinal problems at birth—Children with scoliosis at birth (congenital scoliosis) have a greater risk for worsening of the curve. • Shape (nonstructural scoliosis and structural scoliosis)—A nonstructural scoliosis is a curve that develops side-to-side as a C– or S-shaped curve. This form of scoliosis results from a cause other than the spine itself (e.g., poor posture, leg length discrepancy, pain). A structural scoliosis is a curvature of the spine associated with vertebral rotation. A structural scoliosis involves the twisting of the spine and appears in three dimensions. • Location—The curve of the spine may develop in the upper back area where the ribs are located (thoracic), the lower back area (lumbar), or in both areas (thoracolumbar). • Direction—Scoliosis can bend the spine left or right. • Angle—A normal spine viewed from the back is zero degrees—a straight line. Scoliosis is defined as a spinal curvature of greater than 10 degrees (i.e., bending toward the ground when in the upright position). The degree of the lateral curvature is expressed by the Cobb angle, which is calculated from a radiograph as shown in Figure 24-2. The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Atelectasis (see Figure 9-8) and Excessive Airway Secretions (see Figure 9-12)—the major anatomic alterations of the lungs associated with kyphoscoliosis (see Figure 24-1). CLINICAL DATA OBTAINED AT THE PATIENT’S BEDSIDE CLINICAL DATA OBTAINED FROM LABORATORY TESTS AND SPECIAL PROCEDURES Pulmonary Function Test Findings Moderate to Severe Kyphoscoliosis (Restrictive Lung Pathology) FORCED EXPIRATORY FLOW RATE FINDINGS
Kyphoscoliosis
Anatomic Alterations of the Lungs
Etiology and Epidemiology
Diagnosis
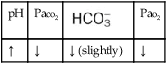
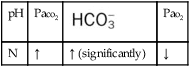
 OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Kyphoscoliosis
OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Kyphoscoliosis
FVC
FEVT
FEV1/FVC ratio
FEF25%-75%
↓
N or ↓
N or ↑
N or ↓
FEF50%
FEF200-1200
PEFR
MVV
N or ↓
N or ↓
N or ↓
N or ↓