56 Kawasaki’s Disease
Etiology and Pathogenesis
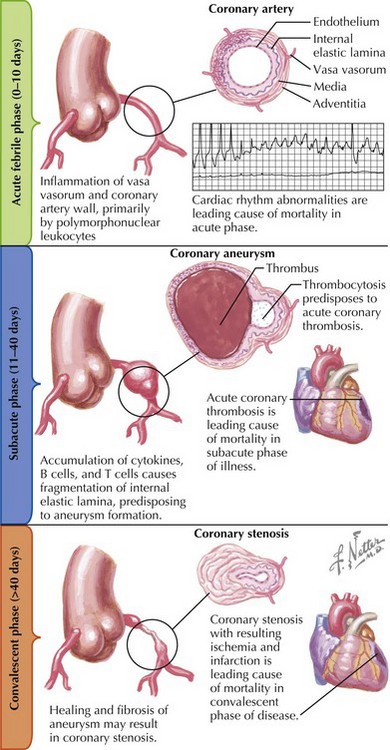
Kawasaki’s disease is a nonspecific vasculitis that affects small- and medium-sized arteries throughout the body. Its most serious consequences evolve in phases within the coronary arteries (Fig. 56-1).
Clinical Presentation
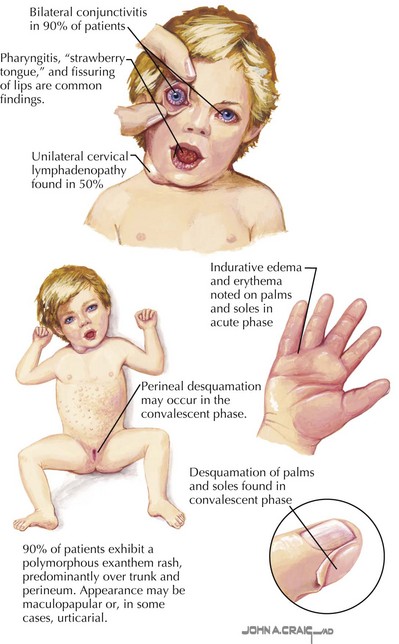
Fever is the cardinal presenting sign of Kawasaki’s disease and persists for more than 7 days in more than 95% of patients. It responds only temporarily to antipyretic therapy and may last up to 2 weeks in patients who are not treated with IVIG. Within 5 days of the onset of fever, 90% of patients develop a polymorphous rash predominantly over the trunk (Fig. 56-2). This may be a diffuse maculopapular rash, or it may be a more urticarial rash. Rarely, perineal desquamation is seen in the subacute phase. Mucosal changes, erythema, and fissuring of the lips occur in 90% of patients. Pharyngitis and prominent papillae (“strawberry tongue”) are also typical signs. Within the first week of the illness, bilateral conjunctivitis, consisting of a discrete vascular injection with absence of corneal clouding or purulent exudates, develops in 90% of patients. The bilateral conjunctivitis persists for 1 to 2 weeks. Anterior uveitis is a common finding on slit-lamp examination. Indurative edema and erythema of the hands and feet occur in 75% to 90% of patients. Desquamation of the fingertips and/or the palms and the soles may occur 2 to 3 weeks after the acute illness. Cervical lymphadenopathy, the least consistent finding, occurs in approximately 50% of patients. It is usually unilateral, and the diameter of the nodes may exceed 15 mm.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


