Fig. 20.1
Joseph Barcroft (1872–1947). Photograph by Bassano Ltd. By permission of the National Portrait Gallery
20.2 Glass Chamber Experiment of 1920
This is one of the most colorful episodes in the history of high altitude physiology. Barcroft was the subject himself, and he lived continuously in a small sealed room for 6 days while subjecting himself to increasingly severe hypoxia. The conditions were heroic. In the process he surrendered about 2.5 cm of his left radial artery, nearly fainted during the blood-drawing procedure needing brandy to revive himself, and all for a result with an n of 1.
20.2.1 Rationale for the Experiment
This is clearly set out at the beginning of the article [6]. The study was a direct response to the claim by John Scott Haldane (1860–1936) that the lung actively secreted oxygen across the blood-gas barrier. Much of the evidence for this came from the Pikes Peak expedition of 1911 that included Haldane and three other physiologists [12], and the results were published in 1913, 7 years before Barcroft’s experiment. The report from that expedition stated that on the first day of the period of a month on the summit, altitude 4300 m, the oxygen partial pressure in the blood exceeded that in the alveolar gas by 7 mm Hg. Furthermore as Barcroft noted, after 2 or 3 more days, and during exercise that doubled the oxygen consumption, the arterial PO2 exceeded that in alveolar gas by an average of 32 mm Hg.
Haldane had originally become interested in the possibility of oxygen secretion by the lung following a visit to Christian Bohr (1855–1911) in Copenhagen. Haldane and Lorrain Smith carried out a series of experiments on animals that seemed to support the secretion hypothesis. Interestingly, Haldane retained his belief in oxygen secretion in spite of mounting evidence against, it throughout his life [22].
Barcroft was not the only person who was skeptical of oxygen secretion but he was determined to test the secretion theory. He pointed out that Haldane and colleagues had calculated the arterial PO2 from the oxygen and carbon monoxide concentrations in the blood after the subject had inhaled a small amount of carbon monoxide, and he argued that this indirect measurement of PO2 might be liable to error. For this reason Barcroft made direct measurements of the oxygen concentration of arterial blood by exposing the blood to a partial vacuum [4]. He then calculated the oxygen saturation, and derived the PO2 from his own oxygen dissociation curve that he had measured in 1910 during an expedition to Tenerife [1].
It should be noted that in spite of this direct challenge by Barcroft to Haldane’s belief, the two men were friends and in fact had previously worked together on methods of measuring the PO2 in small samples of blood [4]. Although Haldane had his base in Oxford and Barcroft was in Cambridge, and Haldane held to the theory of oxygen secretion by the lung for the remainder of his life, these two eminent scientists remained cordial and spoke highly of each other’s work on several occasions.
20.2.2 Background of the Glass Chamber
Barcroft’s procedure of placing humans in a small closed glass chamber where they could inspire an altered oxygen mixture can be traced back to his work on gas poisoning during World War I [3]. Barcroft’s family had been members of the Society of Friends (Quakers) for generations and were therefore non-combatants. Barcroft resolved this dilemma during the war by acting as a civilian attached to the army. One of his studies was to test the effects of poisoned gases in a closed chamber. Chlorine gas was initially used by the German army starting in April 1915 although apparently this new form of warfare did not have the support of the German High Command but came about because of a directive from the Kaiser himself [13]. The initial physiological studies using the chambers were made on rabbits exposed to chlorine or phosgene, but later soldiers who had been gassed in the trenches were treated with about 40–50 % oxygen in the chambers. Interestingly the idea of giving these patients an increased oxygen mixture to breathe was not immediately accepted although today we would automatically use oxygen in the treatment of patients with acute inflammation of the lung caused by a noxious gas.
The glass chambers were relatively small having capacities of 10 or 12 m3 and they were constructed of plate glass supported by iron frames. Three of the chambers could be connected together. Carbon dioxide that accumulated in the chamber was removed by soda lime and excess water vapor was taken out by calcium chloride. Typically the patients remained in the chamber overnight but left it for 8 h during the day. The size of the chamber used in the experiment described here was not given but the photograph (Fig. 20.2) shows that it was large enough to contain a bed and other equipment such as a cycle ergometer [19].
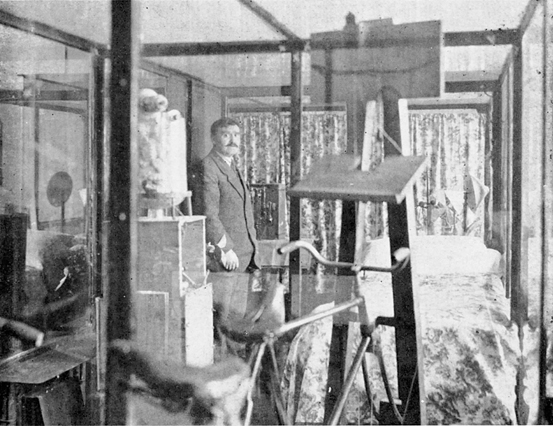
Fig. 20.2
Glass chamber in which Barcroft exposed himself to increasingly low concentrations of oxygen over 6 days. A bed, cycle ergometer and other equipment can be seen. The man is Sergeant-Major Secker who was Barcroft’s longtime assistant. From [13]
In his account of the experiment in 1920, Barcroft contrasts his use of a glass chamber in his laboratory with existing high altitude facilities. For example he describes the Margherita Hut on the Monte Rosa, altitude 4559 m, as “but an improvisation as compared with the modern physiological laboratory”. He goes on to say that “at such places there is usually a certain amount of indigestion, sometimes constipation, sometimes diarrhoea, usually extreme cold. It is therefore open to dispute how far such symptoms as headache are due to disorders not directly connected with anoxemic conditions”. By contrast he claimed that the glass chamber in his laboratory meant that “every sort of convenience was accessible”. However the limited hygiene facilities for a continuous stay of 6 days and nights in his glass chamber suggests that while laboratory equipment was no doubt accessible, the conditions in the chamber must have been spartan.
The long period of 6 days was chosen because Haldane and his colleagues had reported that the oxygen secretion ability of the lung increased over time at high altitude. For the same reason, Barcroft exercised on a stationary bicycle on the last day because this was also reported to increase oxygen secretion. Throughout the 6 days and nights Barcroft’s activities were closely monitored by eleven university students whose names are duly acknowledged at the end of the article. An interesting sidelight was that although the students reported that while Barcroft appeared to sleep well at night, his own belief was different. He stated “My own view of the matter was quite otherwise. I thought I had been awake half the night and was unrefreshed in the morning … the slumber was very light and fitful with incessant dreams” [2].
Nowhere does Barcroft refer to the difficulties of living continuously in the chamber for 6 days although one wonders whether the British stiff upper lip attitude was a factor. He claimed that he “had been thoroughly well fed—a rather light breakfast, tea, eggs, bread and butter cooked by the attendant and lunch and dinner sent from the college kitchens”. An exception was when he awoke on the morning of the 6th day with what he refers to as “the typical symptoms of mountain sickness, vomiting, intense headache and difficulty of vision”. He very reasonably attributed these symptoms to the hypoxia because by then he was at an equivalent altitude of 18,000 ft (5486 m).
20.2.3 Experimental Procedure
Barcroft entered the chamber on February 1, 1920 and the operative procedures to sample arterial blood were carried out during the evening of February 7. When he entered the chamber, the PO2 of the air was given as 163 mm Hg and this gradually fell as nitrogen was pumped in and oxygen was consumed by the subject. Barcroft analyzed the air in the chamber himself throughout the 6 days using a Haldane gas analyzer [14]. The lowest inspired PO2 was 84 mm Hg on the morning of February 7. As stated above this was equivalent to an altitude of 18,000 ft (5486 m) which was far higher than any existing high altitude laboratory at the time. The removal of CO2 from the chamber by soda lime was more efficient at the end than the beginning of the experiment, and during the last 48 h the PCO2 varied from 3 to 5 mm Hg.
The actual surgical procedure is described in detail. The operation on the radial artery began at 7:28 p.m. but by 7:30 to 7:40 it was recorded that the subject was “inclined to be faint” and as a result he was given tea and brandy. As a result he was “sufficiently himself to breathe through valves without the samples being invalid through looseness of grip with the lips”. The left radial artery was exposed for an inch and a half, a ligature was applied to the distal end, and a clip was placed on the proximal end. Then an incision was made in the artery to receive the cannula from which blood was withdrawn. This was done both during rest and exercise on the cycle ergometer, the total volume of blood removed being 83 ml. The exercise protocol was impressive, the total time being 37 min with the work rate varying between 350 and 386 kg m min−1 (57–63 watts). During the blood draws, alveolar gas samples were collected thus allowing the difference between the PO2 in alveolar gas and arterial blood to be measured.
Some details of the operative procedure are puzzling. This must have been carried out in the chamber while Barcroft was exposed to the hypoxia. but it seems unlikely that the person could do the operative procedure when acutely exposed to an altitude of 5400 m. Perhaps he used an oxygen mask, but in this case it would be difficult to avoid contaminating the chamber with oxygen.
20.2.4 Experimental Results
These are described in Sect. 4 of the manuscript with the details given in Table XII. To be frank, the description of the results is not as clear as one would like. First there is a qualitative statement in the first paragraph that might raise eyebrows today. Barcroft stated that with the measured PO2 in the alveolar gas of 57–68 mm Hg, the oxygen saturation of blood with the same PO2 would be expected to be between 80 and 90 %. He then went on to say that when the first sample of arterial blood was drawn, “the blood looked dark” and from this he argued that this was evidence against oxygen secretion since if the PO2 of the blood were a few mm Hg higher than that of the alveolar gas as predicted by Haldane, the blood would be expected to have its usual red color. This is hardly convincing.
Table XII then shows the actual numbers. For the resting subject, the alveolar PO2 is given as 68.4 mm Hg. This comes from a procedure that Barcroft referred to as the Krogh method, and consisted of collecting the last 2 ml of gas from each of a series of expirations in a glass tonometer. This value was then compared with the calculated arterial PO2 of 60 mm Hg. This PO2 was derived from the measured arterial oxygen saturation of the blood sample and then using a previously determined oxygen dissociation curve from Barcroft’s own blood [1]. In this way for the resting subject the arterial PO2 was calculated as 8.4 mm Hg less than the alveolar value.
For the exercising subject, the alveolar PO2 was given as 56.5 mm Hg using the Krogh technique but 54 mm Hg using a slight modification of this called the Haldane method. The PO2 in arterial blood was again calculated from the measured oxygen saturation and oxygen dissociation curve and the value was 48 mm Hg. Therefore the arterial PO2 was some 6–8 mm Hg lower than that in alveolar gas. Barcroft went on to say that the disparity between the PO2 in alveolar gas and arterial blood was greater during work than during rest although the actual numbers do not seem to support this.
Barcroft then calculated what he called the “diffusion constant” during work. This was done by dividing the measured oxygen consumption of 750 ml per minute by the alveolar-arterial PO2 difference. The value was given as 107 ml (actually 107 ml min−1 mmHg−1). However the basis of this calculation is questionable because the PO2 of the blood in the pulmonary capillary during the loading of oxygen is not the arterial value but the gradual transition between the PO2 of mixed venous blood and the arterial blood.
It was concluded that the results of these experiments disproved Haldane’s secretion theory because both at rest and during exercise the arterial PO2 was less than the alveolar value. But in the final paragraph of the manuscript Barcroft gallantly remarked “We yield to none in appreciation of the accuracy of the work on this subject of oxygen secretion published by Haldane and his colleagues, and we cannot but think that the difference between us and them has to be sought in the assumptions which Haldane makes, rather than the accuracy of his observations”.
The reader of today comes away from this paper with somewhat conflicting emotions. Clearly this was a heroic experiment entailing what must have been 6 grueling days in a small enclosed space with the unpleasantness of the worsening hypoxia, not to mention the loss of one radial artery. On the other hand the method of measuring the arterial PO2 was questionable with the value being derived from an oxygen dissociation curve measured several years previously. Perhaps the biggest limitation of all was that only two measurements were made, one at rest and another at exercise, and in only one subject. It is easy to imagine that Barcroft was looking for an opportunity to obtain additional data, and this was provided by the expedition to Cerro de Pasco that is described below. However before moving to that here is a brief description of another remarkable experiment carried out by Barcroft in one of his glass chambers.
20.3 Toxicity of Hydrocyanide Gas
As indicated earlier, Barcroft worked on gas poisoning during World War I. One of the gases being considered was hydrogen cyanide (HCN) and Barcroft volunteered to test the effects of this gas on himself and a dog. Although the experiment was carried out in 1917, the full report was published until 1931 [3].
Barcroft and a dog weighing about 12 kg were simultaneously exposed to an atmosphere containing a concentration of what was estimated to be 1 part in 2000 of hydrogen cyanide gas in air. The results of the experiment were set out in Table V which is reproduced here as Fig. 20.3. As the table shows, the dog became unsteady by 50 s and was unconscious by 1 min and 15 s. By 1 and a half minutes it developed tetanic convulsions and was thought to be nearly dead. A few seconds later Barcroft came out of the chamber, put on a respirator, and removed the dog. Five minutes after the initial exposure Barcroft felt a brief period of nausea and a little later noticed difficulty in maintaining attention during conversation. As the note at the bottom of the table indicates, the apparently dead dog was set aside for burial but in fact was found walking around next morning and fully recovered.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


