Fig. 1.1
An ECG at rest showing a narrow complex tachycardia of rate. Although the P wave appears immediately before the QRS, the rhythm is not sinus as the P wave axis is inverted (negative in lead II, III and aVF)
His 24-h tape confirmed a persistent tachycardia, continually starting and stopping throughout the 24 h, and vagal manoeuvres performed during the tape reproduced the sensation of a “kick” in his chest and showed termination of tachycardia (Figs. 1.2 and 1.3). The differential diagnosis was atrial tachycardia or permanent junctional reciprocating tachycardia (PJRT). This was discussed with the patient and his parents. A two-dimensional echo showed no structural abnormalities, and his function was within normal limits.
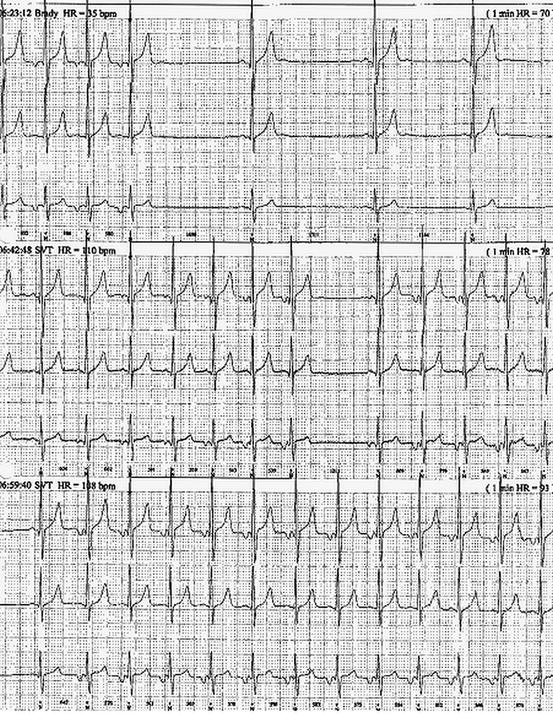
Fig. 1.2
Section of 24-h tape displaying the persistent nature of this tachycardia
Fig. 1.3
Further sections from the 24-h tape showing in more detail the tachycardia stopping and restarting. The tachycardia appears to stop in the retrograde limb i.e. the accessory pathway limb of the re-entrant circuit. Atrial tachycardia could not be ruled out but was felt unlikely from the short PR interval
After counselling he underwent diagnostic electrophysiological study and catheter ablation. At electrophysiological study performed with propofol, the tachycardia was easy to see. The re-entrant nature of the tachycardia was confirmed and the retrograde limb of the circuit mapped characteristically to the mouth of the coronary sinus. The findings were consistent with PJRT. The VA interval was long in tachycardia as predicted, but when the earliest VA interval was identified, radiofrequency energy was applied and the tachycardia terminated. Thereafter tachycardia was not inducible despite pacing manoeuvres and isoprenaline. He made a prompt and uncomplicated recovery. Further follow-up has shown that the ablation has cured the condition and he is symptom-free with no evidence of tachycardia recurrence on 24-h monitoring.
Discussion
Permanent Junctional Reciprocating Tachycardia
PJRT is a rare type of atrio-ventricular (AV) re-entrant tachycardia. There is antegrade conduction through the AV node and slow retrograde conduction through a concealed accessory pathway. The retrograde pathway is often located at the mouth of the coronary sinus posteriorly. Microscopically the pathway has been described as having a serpiginous appearance, which may account for the delayed conduction through it. The pathway cannot conduct antegradely from atrium to ventricle and so there is no delta wave. PJRT is thought to account for around 5 % of childhood supraventricular tachycardia (SVT) and can present at any time from the foetal period until adulthood. It has been suggested that the majority of patients present during the first year of life, but cases can often present in later childhood.
The slow retrograde conduction facilitates the installation of this arrhythmia, which is often incessant from infancy, with few intermittent periods of sinus rhythm. The ventricular rate is variable, and whilst it can be over 250 bpm in neonates may also be seen at rates of 100–150 bpm in adolescents.
Clinical Presentation and Diagnosis
As the tachycardia may be persistent, and relatively slow, it can be relatively well tolerated. Syncope, for this reason, is unusual. Palpitations may not be recognised and if undiagnosed for prolonged periods, patients may present with fatigue or heart failure, which can result in a dilated cardiomyopathy. Whilst not so in our case, some patients have presented in the advanced stages of heart failure and have only been recognised when on the list for transplantation.
PJRT is diagnosed by a standard 12-lead electrocardiogram (Table 1.1).
Table 1.1
ECG alterations in PJRTa
Rhythm | Regular, can be confused with sinus tachycardia as the p wave is just before the QRS |
Rate | Tachycardia, varies with age but may not be as rapid as “normal SVT” |
P wave | Negative P wave in inferior leads, reflecting low atrial origin < div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|