Ischemic Heart Disease
Careful transesophageal imaging can reveal a great deal of information about the anatomy of the coronary tree. The presence of stenosis is indicated by the compromise of the lumen. To be certain that what is being imaged is truly a stenosis rather than an artifact produced by an oblique section through the vessel, it is necessary to be able to see normal lumen on either side of the obstruction. Poststenotic dilatation may be present; it suggests a severe stenosis. Other markers of severe stenosis are an elevated pressure gradient across the stenosis by conventional Doppler and the presence of turbulence in the region of the stenosis on color-flow Doppler. The use of echocardiographic contrast may enhance flow visualization. Additional segments of the coronary vessels may be visualized and stenosis identified in these segments following contrast injection. The left main and proximal segments of the left anterior descending, left circumflex, and right coronary arteries, together with some of their branches, can be visualized by transesophageal echocardiography. With newer color Doppler equipment, smaller epicardial and intramyocardial vessels (e.g., septal perforators) can also be seen.
Wall motion abnormalities are also well visualized by transesophageal echocardiography, especially using the transgastric approach. Mitral regurgitation in ischemic heart disease can be recognized and its severity assessed. Mitral annular dilatation and dilatation of the left atrium and left ventricle imply long-standing, significant mitral regurgitation. When the head of the papillary muscle is ruptured, it can often be imaged prolapsing into the left atrium. In up to 30% of patients, however, the ruptured head may not prolapse into the left atrium. In these cases the diagnosis is made by observing the chaotic movement of the ruptured head in the left ventricle. Meticulous examination is important in these cases.
The term pseudoaneurysm refers to a rupture of the ventricle that is walled off by a clot before the patient experiences fatal tamponade. These lesions have a narrow neck (which distinguishes them from true aneurysms) that leads to a walled-off cavity. Pseudoaneurysms are inherently unstable in that they have a propensity to rupture. They should be resected even if discovered late after a myocardial infarction in an otherwise stable patient.
Other mechanical complications that can result from ischemic heart disease include ventricular septal rupture, which is easily seen on color-flow Doppler. Posterior ventricular septal defects are often best visualized using the transgastric approach.
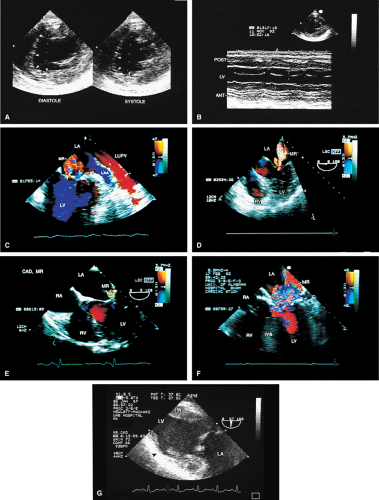 FIGURE 6.3. Left ventricular dysfunction. A. Marked hypokinesis of the anterior septum (arrowheads) is seen in this patient with ischemic heart disease. The inferior wall is also hypokinetic. B. M-mode image from the same patient shows hypokinesis of anterior (ANT) and inferior walls (POST). C. Color Doppler examination in this patient demonstrates two mitral regurgitation (MR) jets resulting from left ventricle (LV) dysfunction. D. Another patient with moderate MR resulting from ischemic heart disease. E,F. Two other patients with mild (E) and severe (F) MR. Because the mitral valve (MV) leaflets appear to be structurally normal, the MR is presumed to be ischemic in origin. In both patients the LV and the mitral annulus were enlarged. G. Dyskinesis of the LV anterior free wall (black arrow) in this transgastric systolic frame in another patient. IW, LV inferior wall. IVS, ventricular septum. LA, left atrium; LAA, left atrial appendage; LUPV, left upper pulmonary vein; RA, right atrium; RV, right ventricle. |
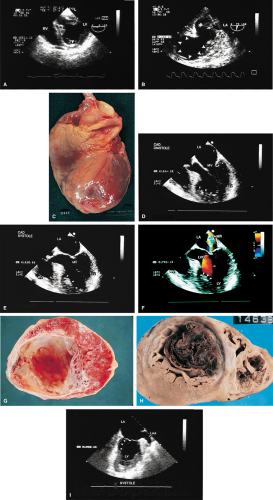 FIGURE 6.4. Left ventricular apical aneurysm. A. A bright, fibrotic scar (arrowhead) in the aneurysmal apex. B. A huge left ventricular (LV) apical aneurysm (arrowheads). C. Gross specimen of LV apical aneurysm caused by an acute myocardial infarction. D–F. Another patient with a large apical aneurysm containing a thrombus (arrowheads). F. Color Doppler examination shows the presence of associated mitral regurgitation (MR). G,H. Gross specimens of LV aneurysm with mural thrombus. I. Aneurysmal proximal inferior wall (arrowheads) is seen in the two-chamber view. Note the myocardial thinning, which is well seen. LA, left atrium; LAA, left atrial appendage, LVO, left ventricular outflow tract; MV, mitral valve; RV, right ventricle. |
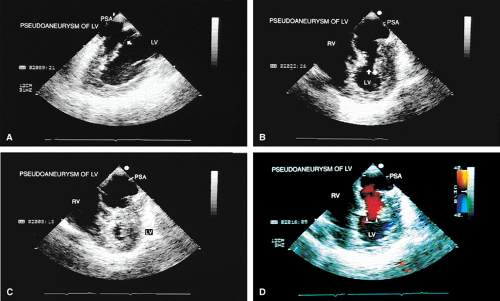 FIGURE 6.5. Left ventricular pseudoaneurysm. The arrows in A and B show the communication of the left ventricle (LV) with a large pseudoaneurysm (PSA). In B and C the pseudoaneurysm appears to be larger than the LV cavity. D. Color Doppler examination reveals flow signals moving from the LV into the PSA through the relatively narrow neck (arrowheads). Pseudoaneurysms are differentiated from true aneurysms by their narrow necks; in pseudoaneurysms the neck or mouth is smaller than the aneurysm cavity, whereas in true aneurysms the mouth or neck is much larger, often as large as or larger than the cavity. RV, right ventricle. |
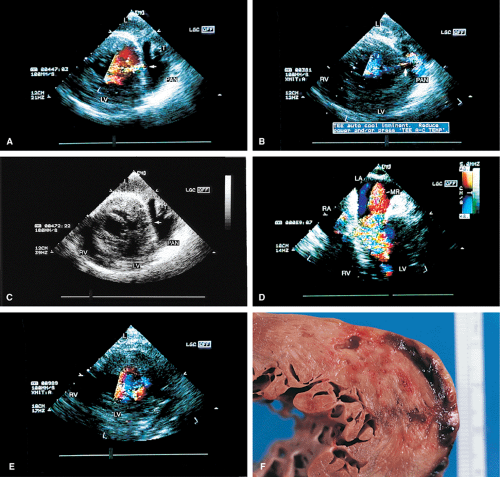 FIGURE 6.6. Contained slit-like cardiac rupture following acute myocardial infarction. A–E. Transgastric views (A,B) show a large and narrow color jet (arrow) within the left ventricle (LV) posterior wall. B also shows color-flow signals partially filling the pseudoaneurysm cavity (PAN). In C, the color Doppler was turned off, revealing an echo-free space (arrow), which corresponded to the site of the color jet seen in A; however, it could not otherwise be distinguished from an artifactual echo “dropout.” Associated moderate mitral regurgitation (MR) is noted in D. E. Postoperative image shows absence of color-flow signals within the myocardial wall. F. Gross specimen from another patient shows a contained LV rupture. LA, left atrium; RA, right atrium; RV, right ventricle. (A–E reproduced with permission from Rao A, Garimella S, Nanda NC, et al. Transesophageal color Doppler echocardiographic diagnosis of cardiac rupture following acute myocardial infarction. Echocardiography 1996;13:309–312. ) |
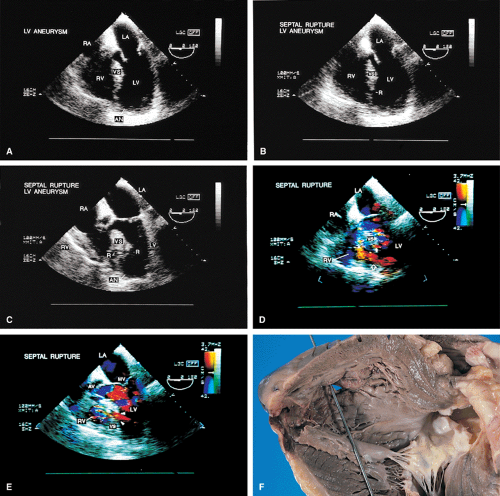 FIGURE 6.7. Ventricular septal rupture. A–C. Ventricular septal rupture (R) with an apical aneurysm (AN). D,E. Color Doppler examination shows shunting of flow across the ruptured interventricular septum into the right ventricle (RV) (arrows). F. Gross specimen from another patient shows a probe passing through a ruptured ventricular septum (VS). LA, left atrium; LV, left ventricle; MV, mitral valve; RA, right atrium; RV, right ventricle. |
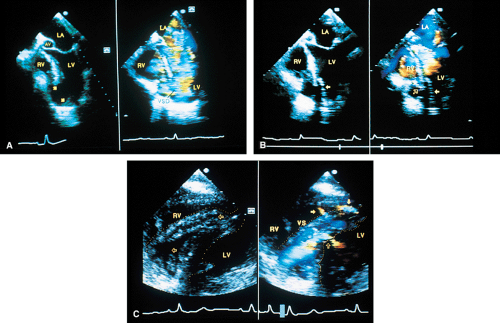 FIGURE 6.8. Ventricular septal rupture after acute anterior myocardial infarction. A. Apical five-chamber view. Flow signals are seen moving from the left ventricle (LV) into the right ventricle (RV) through the large apical defect (arrows). B. The patch (solid arrow) used to close the defect. C. Transgastric views (transverse plane imaging) from the same patient show marked enlargement and widening of the ventricular septum (VS), with large areas of echolucency consistent with dissection (horizontal open arrows in C). Color Doppler imaging shows prominent color-flow signals (maximal width 10 mm) moving from the LV into the ventricular septum (VS) (vertical open arrow in C) and occupying the large echolucent areas seen on the non-color Doppler image. The prominent area of localized relatively high-velocity signals (flow acceleration) noted in the LV measured 9 mm at the site of the defect. No corresponding defect at the same level is seen on the right ventricular aspect, but two smaller sites of rupture, both 5 mm in size, are noted on the right side further posteriorly (solid arrows in C). These are associated with smaller areas of flow acceleration (1.5 to 2 mm). These defects are not delineated on the two-dimensional image, but are visualized only during color Doppler examination. Therefore, the patient has four defects in the VS, one very large and located in the apical region, and the other three much smaller and located more posteriorly. None of the findings noted in C were demonstrated by transthoracic echocardiography. VSD, ventricular septal defect. LA, left atrium. (Reproduced with permission from Ballal RS, Sanyal RS, Nanda NC, et al. Usefulness of transesophageal echocardiography in the diagnosis of ventricular septal rupture secondary to acute myocardial infarction. Am J Cardiol 1993;71:367–370. ) |
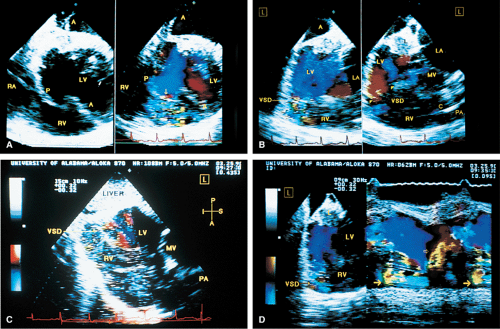 FIGURE 6.9. Ventricular septal rupture after acute inferior myocardial infarction. Transgastric views. A. Transverse plane imaging demonstrates mosaic color signals indicative of turbulent blood flow moving from the left ventricle (LV) through the posterior ventricular septum (P) into the right ventricle (RV). The arrow indicates a localized area of increased velocity with aliasing (flow acceleration) on the left ventricular side of the defect. Note that the defect is not identified on the non-color Doppler two-dimensional image. Top A
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|