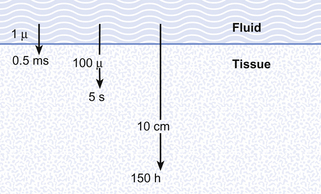
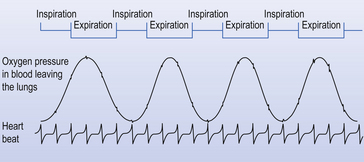
1 The ‘bottom line’ of an account of the complicated process of respiration begins with a flow of One definition of the success of a species of organism, in evolutionary terms, is how well it can maintain constant the composition of the fluid surrounding its individual cells (its internal environment) despite changes in its external environment (surroundings getting dryer, colder, warmer etc.). This process is called homeostasis and requires energy. Most of the energy generated by our tissues is the result of oxidation of food substrates, and this is the reason we need a flow of OXYGEN IN. Neophytes in physiology often emphasize the role of the respiratory system in providing this oxygen, and certainly an uninterrupted supply is important, particularly for the nervous system, but of more immediate importance is the removal of CO2. The word oxygen means ‘acid producer’ (Greek, oxy; acid; gen, to produce), and the major product of our oxidative metabolism is the acid gas CO2. The accumulation of CO2 would result in acidification of the body fluids. The importance of removing this CO2 can be demonstrated by rebreathing from a plastic bag for a few minutes. The unpleasant sensation that forces you to stop this rather dangerous experiment is due to over stimulation of the reflex that controls breathing to get rid of this gas. You will see later (Chapter 8) that CO2 produces its acidic effect by reacting with water to form carbonic acid. Although in human beings the same passive mechanism of diffusion alone supplies and removes these gases from our bodies (there is no active chemical transport), the phenomenon of diffusion is maximized by complicated respiratory and circulatory systems which accomplish what the pond water does for the amoebae in providing a supply of and a sink for these gases. The lungs promote diffusion by having an enormous surface area, which is very thin, through which diffusion can take place easily. A surface of over 90 m2 is enclosed in a lung volume of less than 10 L. This functional 90 m2 is often reduced in disease, by thickening of the membrane, excess fluid in the lungs, or by a reduction in the supply of air or blood. The circulation of the blood forms the transport link between the diffusion site of the lungs and the diffusion site of the capillaries within the tissues. The distances involved in this link are enormous in molecular terms, and diffusion would be totally useless to transport gas over the metre or so between the lungs and distal tissues of our bodies. This transport is accomplished in seconds by the circulation (Fig. 1.1). The processes of breathing and the beating of the heart are both cyclic events. One involves the inhalation of air and then its exhalation; the other involves filling of the heart with blood and then its ejection into the circulation. The time courses of these two cycles are very different: at rest you may take 12 breaths in the minute the heart beats 60 times, ejecting 5 L of blood through the lungs (see Fig. 1.2).
INTRODUCTION
What is respiration?
The need for respiration
Diffusion in respiration and the circulation
Timing in the circulation and respiration
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine