(1)
Anatomy Department, University of Medicine and Pharmacy Carol Davila, Bucharest, Romania
Abstract
The right atrium is situated in front and to the right from the left atrium. From the tricuspid orifice the right atrium is located further more behind than above (Fig. 6.1).
6.1 Internal Configuration of the Right Atrium
The right atrium is situated in front and to the right of the left atrium. From the tricuspid orifice the right atrium is located further more behind than above (Fig. 6.1).
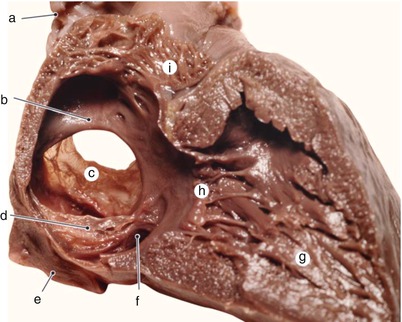
Fig. 6.1
Five months old heart. Sagittal paramedian section through the right heart. a superior vena cava b septum secundum, c septum primum, d inferior vena cava valve, e inferior vena cava, f sinus ostium, g right ventricle, h tricuspid valve, i right auricle
The right atrium has a globular aspect. It has an anterior extension called the right auricle.
The right atrium is where the superior vena cava, the inferior vena cava and the coronary sinus end. The anterior and small veins of the heart (also known as the thebesian veins) open in the right atrium through orifices called foramina thebesii. Through the right atrioventricular orifice – the tricuspid orifice, the blood from the right atrium passes into the right ventricle.
The internal surface of the right atrium has some specific areas:
The right auricle is the anterior expansion of the right atrium, with a general conical shape, deriving from the primitive atrium. The conical shape with the blunt apex, relatively smooth margins and a large base, represent the elements which help in imagistic identification of the right atrium.
The pectinate part is a segment in the wall of the atrium which has the pectinate muscles. They are arranged as muscular trabeculae like “the teeth of a comb”. Actually, this part represents the base of the auricle (Fig. 6.2).
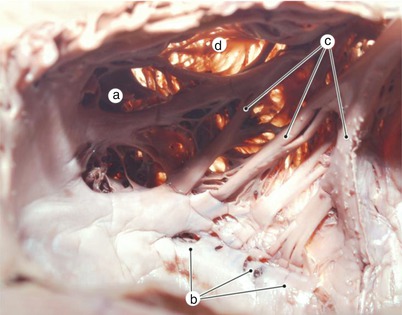
Fig. 6.2
Muscular trabeculae inserted on the inferior segment of the crista terminalis. In the subauricular vestibule a deep venous canal with incomplete wall is observed. a right auricle, b profound venous canal, c muscular trabeculae, d transparent membranous wall
The aspect of the trabeculae in the lumen of the right auricle is highly variable. Frequently one sagital trabecula acts as a support for the insertion of other trabeculae arranged like “the ribs of a palm leaf”. Figures 6.3, 6.4, 6.5, 6.6, 6.7, 6.8, 6.9 and 6.52 offer an exemplification of the variability of pectinate muscles.
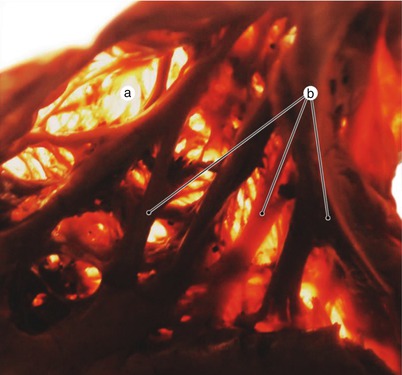
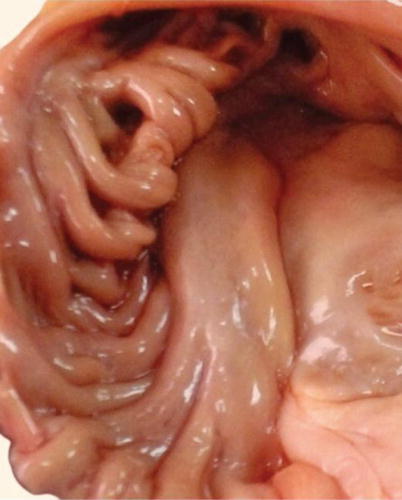
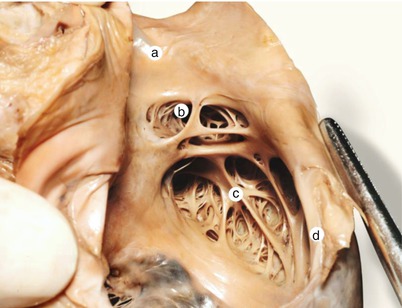
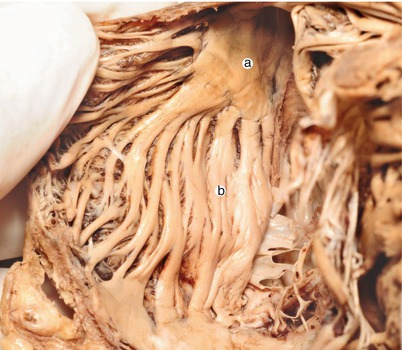
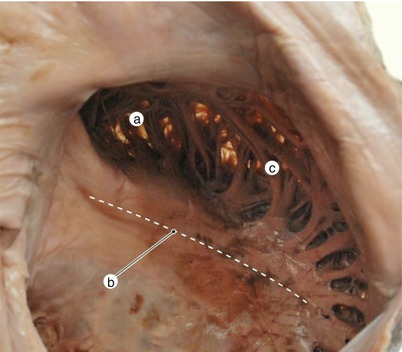
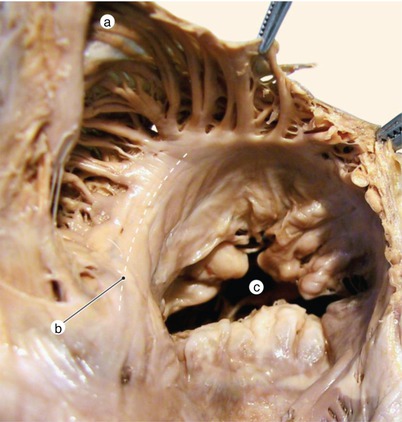
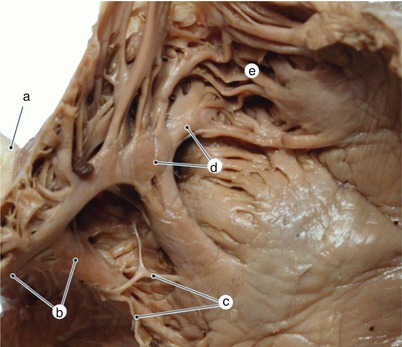
Fig. 6.3
The pectinate muscles – transillumination. The main muscular fascicles, disposed parallelly, like the teeth of a comb. Between these fascicles thinner fascicles anchor the atrial wall which has a membranous appearance. a Transparent membranous wall, b muscular trabeculae
Fig. 6.4
The appearance of the pectinate muscles on a heart not preserved in formaldehyde
Fig. 6.5
Right atrium with the pectinate territory reduced. a superior vena cava, b right auricle, c muscular trabeculae, d terminal ridge
Fig. 6.6
Pattern of organization of the pectinate muscles without connection to the crista terminalis. The pectinate fascicles diverge fanwise, from a common muscular mass, located in the sinus area. a common muscular mass, b pectinate fascicles
Fig. 6.7
Pattern of organization of the pectinate muscles, located backward to the previous case – muscular fascicles reunite on the lateral side of the atrial vestibule. a right auricle, b subauricular vestibule, c pectinate muscles
Fig. 6.8
The insertion of the pectinate muscles occupies approximatively half of the circumference of the tricuspid vestibule. The subauricular vestibule is individualized as a smooth area at the base of the auricle. a right auricle, b subauricle vestibule, c tricuspid valve
Fig. 6.9
Sagittal trabecula in the lumen of the right auricle. In the proximity of the crista terminalis remainings of the right valve of the primitive sinus venosus can be observed. a superior vena cava, b crista terminalis, c remainings of the right valve, d sagital trabecula, e right auricle
In the internal configuration of the right atrium there is a second set of thin trabeculae, harder to identify, situated between the superior part of the crista terminalis and the membranous wall of the primitive atrium. These trabeculae are in continuity with the superficial muscular fibers of the atrium Fig. 6.10.
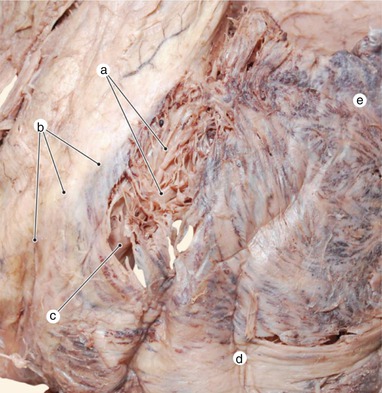
Fig. 6.10
Thin trabeculae diverge towards the atrial wall from the thickness of the crista terminalis, in the proximity of the sinus area. Some of them continue with subepicardial atrial muscle fibers. a thin muscular trabeculae, b terminal sulcus, c crista terminalis, d subepicardial muscular fibers, e right auricle
The sinusal part – called sinus venarum is represented by the smooth surface between the ostia of the two venae cavae (Fig. 6.10).
The tricuspid vestibule derives from the atrioventricular canal. It has an anterior part with smooth walls which can be named the subauricular vestibule.
The floor of the atrium, the cavotricuspid isthmus. The subeustachian and subthebesian sinuses, Koch’s triangle, represent the parts of the vestibule
The atrioventricular septum is represented by the superior segment of the membranous septum
The dorsosinusal space and the interatrial septum with their complex origin
The oval fossa
The valve of the inferior vena cava, which derives from the right valvule of the embryo’s venous sinus
The crista terminalis
Each of these regions alongside other elements present inside the atrium will be defined and described one at a time (Figs. 6.11 and 6.12).
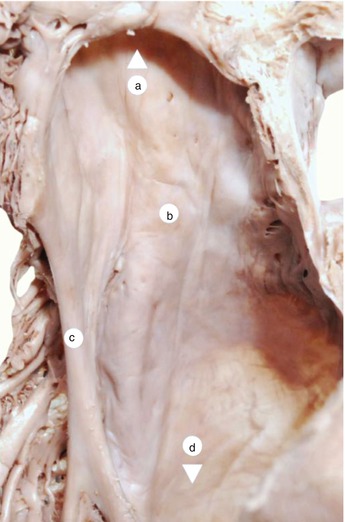
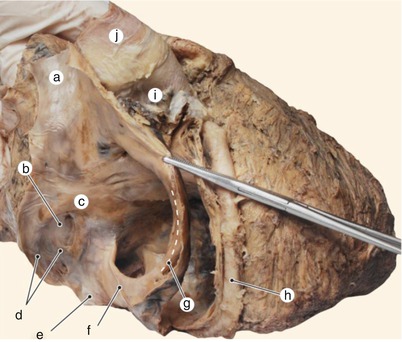
Fig. 6.11
Sinus venarum seen from the interior of the right atrium. a superior vena cava (arrowhead), b sinus venarum, c crista terminalis, d inferior vena cava (arrowhead)
Fig. 6.12
Right atrium after removing the pectinate part. The inferior vena cava orifice is limited anteriorly by a fold with membranous aspect, named the inferior vena cava valvule. a superior vena cava, b fossa ovalis, c limbus, d remainings of the left valve, e inferior vena cava, f inferior vena cava valvule, g crista terminalis, h right coronary artery, i right auricle, j aorta
6.1.1 The Orifice of the Inferior Vena Cava, the Eustachian Valve, Chiari’s Network
The orifice of the inferior vena cava is inconstantly bordered in its front part by an incomplete semilunar valve. This is called the valve of the inferior vena cava or Eustachio’s valve and it derives from the right valve of the embryonic venous sinus (Fig. 6.14). This valve previously directed the venous blood to the interatrial communication, in fetal life.
The valve of the inferior vena cava has variable aspects and dimensions. It covers (and sometimes overlaps in the superior part) a ridge called the Eustachian margin (Figs. 6.13 and 6.14).
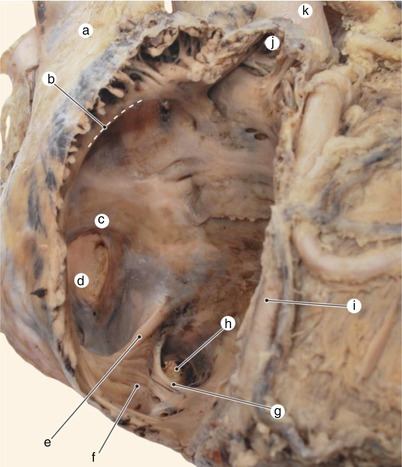
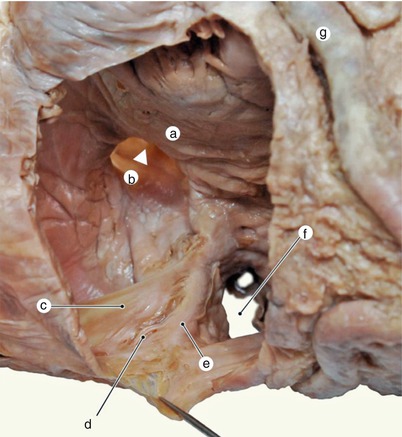
Fig. 6.13
Eustachian edge continues the crista terminalis in its inferior portion. a superior vena cava, b crista terminalis, c limbus, d fossa ovalis, e eustachian edge, f subeustachian sinus, g thebesian edge, h coronary sinus ostium, i right coronary artery, j right auricle, k aorta
Fig. 6.14
The relation between the inferior vena cava valvule and the Eustachian edge. The pectinate atrial wall has been resected. a limbus, b patent interatrial orifice (arrowhead), c inferior vena cava valvule, d cristovalvular recess, e eustachian edge, f coronary sinus ostium, g right coronary artery
The valve of the inferior vena cava usually has a right horn oriented towards its superior part and a left horn oriented towards the septum (Fig. 6.1).
The right horn inconstantly follows the contour of the crista terminalis, and can be more or less individualized. Its extensions with a membranous aspect end before and to the right of the orifice of the superior vena cava (Figs. 6.16 and 6.27a).
In some cases some portions of the right valve of the venous sinus persist into adult life with variable shapes, like a perforated membrane, strips or anastomosed endocardic fascicles. This residual structure is called Chiari’s network (Figs. 6.15, 6.16, 6.17 and 6.18). Its insertion and rapport with the Eustachian margin offer indications about the embryological disposition of the right valve of the venous sinus.
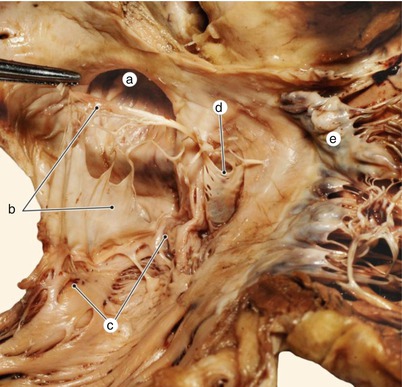
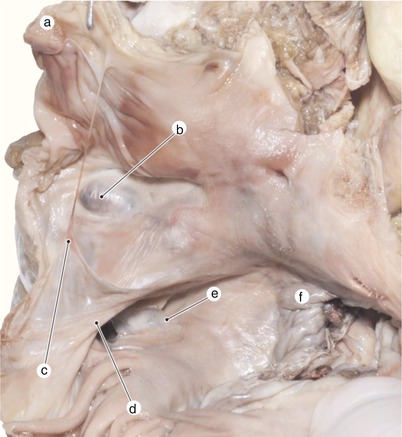
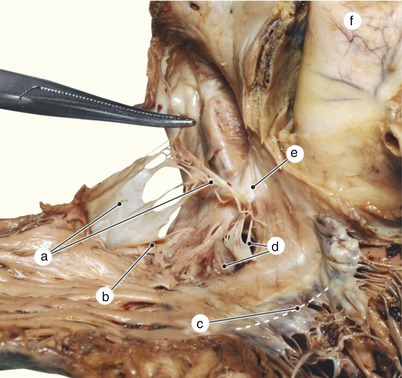
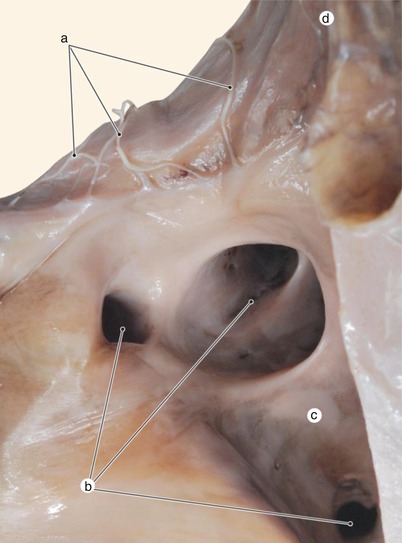
Fig. 6.15
Sinus valvule of muscular origine has been resected. At the point where the Eustachian edge passes under the former right valve a separation is produced between the two valvulae – caval valvula and sinus valvula. a fossa ovalis, b Chiari network – remaining of the right valve, c eustachian edge, d sinus valvule (Thebesian valvule), e tricuspid valve
Fig. 6.16
In adult heart, the limits of insertion have been kept from the right valve of the sinus venosus, reunited by a fibrous bridle. Therefore, we have an image of the initial expansion of the right valve. a superior vena cava, b fossa ovalis with intraseptal tumor, c Chiari network – remaining of the right valve, d eustachian edge, e sinus valvule (Thebesian), f tricuspid valve
Fig 6.17
Inferior vena cava valvule with Chiari’s network. Notice the fact that there are two valvulae of the coronary sinus, each one with clearly different origins. Notice the insertion of the network on the septum secundum. The atrial wall is removed. a Chiari’s network – remaining of the right valve, b eustachian edge, c tricuspid valve, d 2 sinus valvulae, e insertion on the septum secundum, f aorta
Fig. 6.18
Inferior vena cava is opened below and transdiaphragmatic. We can observe the line of insertion of a Chiari’s network at the borderline between the venous endothelium and the atrial endocardium. a Chiari’s network – remaining of the right valve, b hepatic veins orifices, c inferior vena cava, d right atrium
We also can observe that the right valve forms creases as it passes over the Eustachian margin, and its apex reaches the septum secundum.
Observing the continuity between the valve of the inferior vena cava and the valve of the coronary sinus, the common origin of the two structures is confirmed, both deriving from the right valve of the venous sinus (Figs. 6.15, 6.16, 6.17 and 6.18).
Keep in mind:
Chiari’s network could represent the starting point of an intraatrial thrombus. Fragments from this thrombus could migrate to the left atrium through a interatrial septum defect, which is a frequent finding alongside Chiari’s network. These fragments could give birth to paradoxical embolisms.
When the right valve has a great degree of remanence in the form of a fibromuscular membrane, it partially divides the right atrium into two sides, situation known as cortriatriatrum dextrum-34 (cortriatriatrum sinister is the situation when the left atrium is divided into two parts by a perforated fibromuscular membrane).
Between the valve of the inferior vena cava and the Eustachian crest there can be reminiscent parts of the cavomarginal recess.
The left horn of the valve of the inferior vena cava is sometimes in continuity with the valve of the coronary sinus (also see embryology).
The latter is represented by an endothelial fold that partially covers the ostium of the coronary sinus in its inferior and right part, preventing the reflux of blood into the sinus.
Sometimes the ostium of the coronary sinus is covered by a valve on its left side.
The valve of the coronary sinus is also a vestige of the right valve of the embryonic venous sinus.
Through the coronary ostium the coronary sinus, the largest collector of the venous coronary system, opens in the right atrium. The coronary sinus derives from the left horn of the embryonic venous sinus.
6.1.2 The Interatrial Septum: Right Surface, the Oval Fossa
The interatrial septum can be considered the left posterior-lateral wall of the right atrium (the right atrium is situated in front and to the right of the left atrium).
In the inferior and posterior part of the septum, at a distance from the atrioventricular orifice, a depression called the oval fossa can be observed.
Its surface is thinner that the rest of the interatrial septum and it is formed in its superior part by the septum primum and in its inferior part by the fusion of these structures:
The septum primum (towards the left atrium)
The vestibular spine
The left valve of the left venous sinus
The fusion of the left valve and the septum primum is variable, and its contour gets more or less disengaged from the floor of the oval fossa.
Sometimes, more frequently in the superior part of the fossa, there is a small interatrial communication, under the form of an oblique orifice cut into the septum. The oblique aspect of the orifice permits the pressure from the left atrium to keep it closed, so that its presence in a small size does not have any hemodynamic significance.
The terms oval foramen or oval window are terms which usually lead to confusion.
Sometimes these terms are used to name an interatrial defect of the septum in the form of a unique orifice in the floor of the oval fossa. In this situation, when the septum primum has united correctly with the septum secundum and there is a relatively circular orifice at the level of the floor of the oval fossa, its correct name should be second orifice-type defect in the floor of the oval fossa (Fig. 6.29).
Other times it refers to the interatrial communication in embryonic life when the term oval foramen – Botallo – is used to name the normal gap between the septum primum and septum secundum, which ensures a shunt for pulmonary circulation. This space (also defined as an intraseptal conduct) is not oval and it does not correspond to the oval fossa, but to the space between the falx septi and septum secundum (Fig. 2.13). When falx septi does not fuse to the adult heart, we can speak of a patent interatrial communication, not an oval foramen (Fig. 6.30).
The oval foramen is a transitory appearance in embryonic life, appearing when the oval fossa does not yet have a well constituted floor, because either the septum primum or septum secundum, or both have reduced dimensions and are not yet overlapped (Figs. 2.12, 2.16 and 2.18) (also see embryology). We also emphasize on the fact that the oval aspect is an aspect given by summation, in reality it being an oblique gap and not an oval orifice.
The oval fossa is limited in its superior, posterior and anterior-inferior borders by a prominent margin called the isthmus or limbus of the oval fossa. The limbus has an anterior and a posterior rim. Sometimes the valve of the inferior vena cava extends to the anterior rim of the oval fossa. The limbus represents the margin of the previous septum secundum (Figs. 6.19, 6.20, 6.21, 6.22, 6.23, 6.24, 6.25, 6.26, 6.27, 6.28, 6.29 and 6.30).
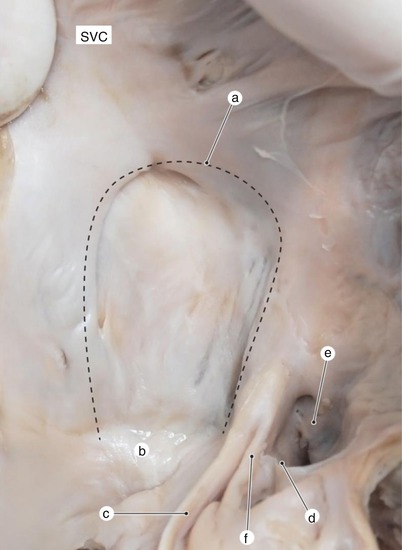
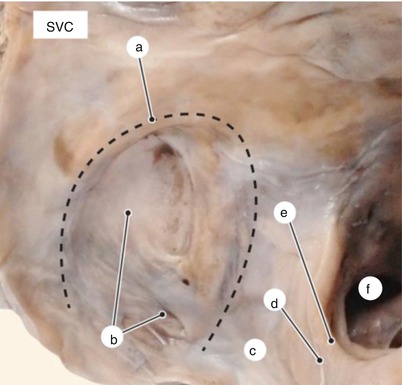
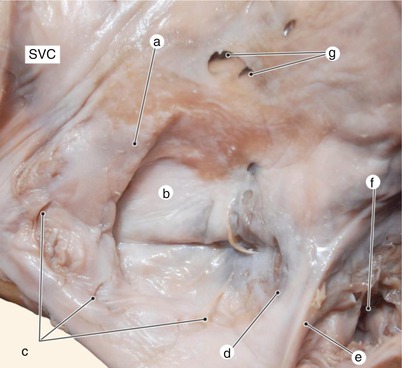
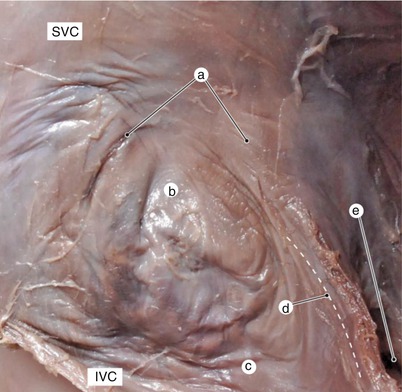
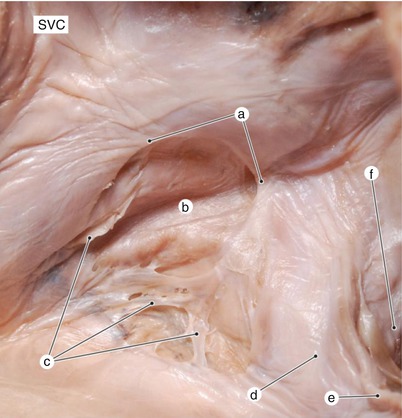
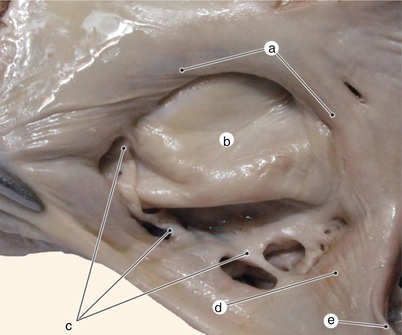
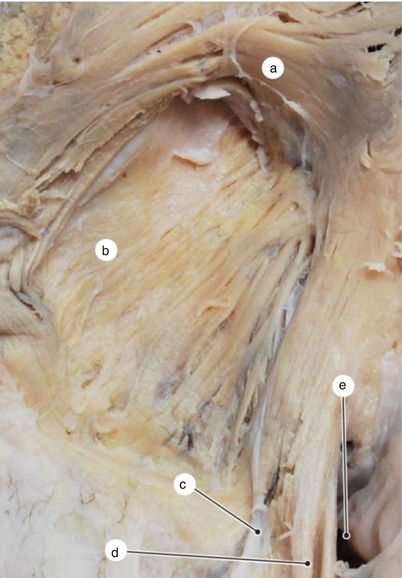
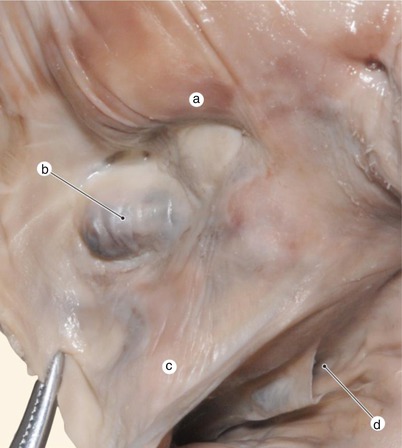
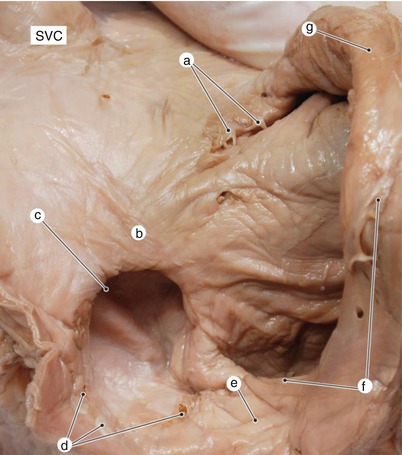

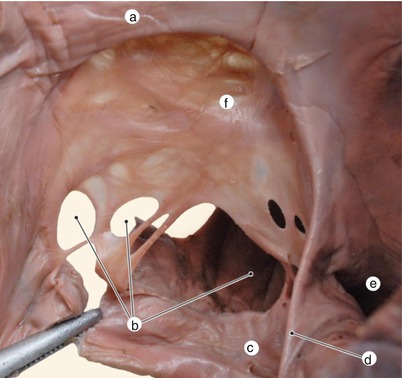
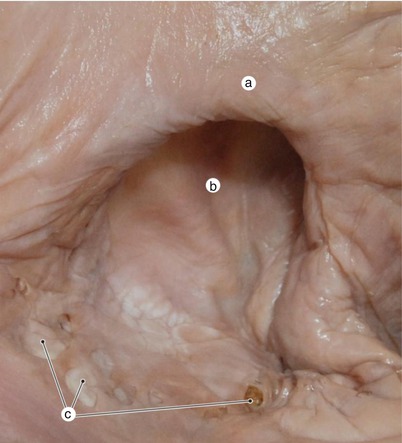
Fig. 6.19
Fossa ovalis. On the Eustachian edge is observed the differentiation between the marginal fold and the fold originating from the sinus septi. SVC superior vena cava, a limbus of the fossa ovalis, b dorsosinusal space, c eustachian edge (marginal fold), d membranous sinus valvule, e coronary sinus ostium, f sinus septi fold
Fig. 6.20
Fossa ovalis with remainings of the left valve. The limbus does not continue with the Eustachian edge. SVC superior vena cava, a limbus of the fossa ovalis, b remainings of the left valve of the sinus venosus, c dorsosinusal space, d inferior vena cava valvule, e eustachian edge, f coronary sinus ostium
Fig. 6.21
Fossa ovalis with remainings of the left valve. Foraminae and foraminules in the superior part of the fossa. SVC superior vena cava, a limbus of the fossa ovalis, b floor of the fossa ovalis, c remainings of the left valve of the sinus venosus, d dorsosinusal space, e eustachian edge, f coronary sinus ostium, g foraminae
Fig. 6.22
Fossa ovalis with weak differentiation of the limbus. SVC superior vena cava, IVC Inferior vena cava. a limbus of the fossa ovalis, b floor of the fossa ovalis, c dorsosinusal space, d eustachian edge, e coronary sinus ostium
Fig. 6.23
Fossa ovalis with remainings of the left valve with coalescence deficiency. SVC superior vena cava, a limbus of the fossa ovalis, b floor of the fossa ovalis, c remainings of the left valve of the sinus venosus, d dorsosinusal space, e eustachian edge, f coronary sinus ostium
Fig. 6.24
Fossa ovalis with formation deficiency of the left valve and the dorsosinusal space. a limbus of the fossa ovalis, b floor of the fossa ovalis, c remainings of the left valve of the sinus venosus, d dorsosinusal space, e eustachian edge
Fig. 6.25
Fossa ovalis with highlighting of the great limbic muscular fascicle. a circle-wise fascicle, b floor of the muscularized fossa ovalis, c inferior vena cava valvule, d eustachian edge, e coronary sinus ostium
Fig. 6.26
Small tumor in the thickness of the fossa ovalis floor. a limbus of fossa ovalis, b small tumor in the thickness of the fossa ovalis floor, c dorsal sinus space, d the coronary sinus ostium
Fig. 6.27
Fossa ovalis arrangement in relation to the terminal crest. Patent interatrial communication. Reminiscences of the left valve. SVC superior vena cava, a right valve reminiscence of primitive sinus venosus, b limbus of fossa ovalis, c fossa ovalis with patent interatrial communication, d left valve reminiscence of primitive sinus venosus, e dorsosinusal space, f valve of the inferior vena cava, g atrial wall folded on the terminal crest
Fig. 6.28
Reminiscence of the left valve at the base of the fossa ovalis. SVC superior vena cava, a limbus of fossa ovalis, b fossa ovalis floor, c left valve reminiscence of the primitive sinus venosus, d dorsosinusal space, e eustachian edge
Fig. 6.29
Orifice secundum type of septal defect in the fossa ovalis floor. Notice the muscularisation of the floor and the fact that the eusctachian edge continues directly with the limbus of fossa ovalis. a limbus of fossa ovalis, b uncompensatede orifice secundum type of septal defect, c dorsosinusal space, d eustachian edge, e the coronary sinus ostium, f fossa ovalis floor partially muscled
Fig. 6.30
Detail of the fossa ovalis that highlights both reminiscence of the left valve and the patent interatrial communication. a limbus of fossa ovalis, b the floor of the oval fossa with patent interatrial orifice, c left valve reminiscence of the primitive sinus venosus
The septum secundum is however a proper septum only in its anterior and inferior borders. Its posterior rim is actually a fold with a fibrous – adipose content derived from the atrium wall (also see embryology) (Fig. 6.31). Even though the posterior rim is initially constituted like a fold it suffers a process of consolidation. As a result, in the adult heart, this segment represents an anatomical and functional segment of the interatrial septum.
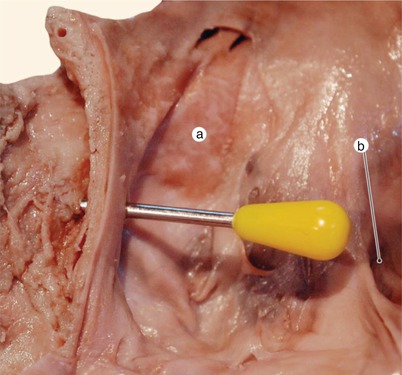
Fig. 6.31
Needle inserted into the limbus of the fossa ovalis through the right atrium, reacheas extracardiac tissue and then perforates the wall of the left atrium. In this way the fold character of the lower posterior part of the limbit is demonstrated. a floor of the fossa ovalis, b coronary sinus ostium
Subendocardially at the level of the limbus, there always is a more or less well-developed circular muscular fascicle of the limbus of the oval fossa (Fig. 6.25).
The limbus of the oval fossa is, however, incomplete in its inferior and posterior parts, where the inferior vena cava seems to be continuing the floor of the oval fossa. In this area, at the endocardial level, we can observe reminiscent parts of the left valve of the embryonic venous sinus with the septum primum. These reminiscent parts are the result of a defect in fusion between the two structures and they appear in variable forms, such as endocardial perforations, rudimentary network, fused membranes, and so on. However, the superior concave aspect of the left valve of the venous sinus can always be spotted. Sometimes, the inefficiency of the fusion between the valve and septum is so obvious that we can consider it a “real Chiari’s network of the left valve” (Figs. 6.20, 6.21, 6.23, 6.24, 6.28 and 6.30).
6.1.3 The Dorso-Sinusal Region
The dorso-sinusal region is the part of the right atrium wall which lies dorsal to the terminal part of the coronary sinus. It derives from the incorporation of the right horn of the primitive venous sinus, the left valve and the sinus septi into the atrium wall.
The endocardium of this region continues the endocardium from the posterior- inferior part of the oval fossa.
The region is bounded in front by the Eustachian margin, behind by the ostium of the inferior vena cava and to its left by the interatrial septum, precisely the posterior inferior part of the oval fossa.
To its exterior, in the area of the crux cordis, it has a corresponding triangular space (the projection of the dorso-sinusal space – term proposition) which is bounded by the contour of the coronary sinus and the inferior vena cava (Fig. 6.32).
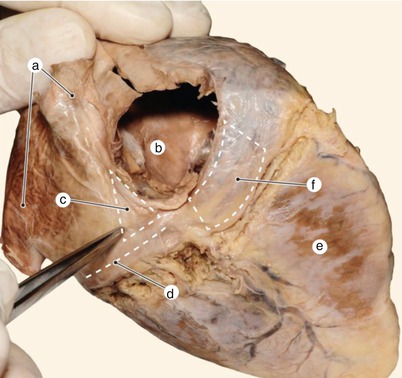
Fig. 6.32
Demonstration of the projections for the venous-tricuspid isthmus and dorsosinusal space. a inferior pulmonary veins, b inferior vena cava, c the projection of the dorsosinusal space, d coronary sinus, e right ventricle, f projection of the venous-tricuspid isthmus
For better understanding of the dorsosinusal space anatomy, it is necessary to review the embryological concepts of the atrial division (also see embryology). Figures 6.33, 6.34 and 6.35 exemplify the dissection of the dorsosinusal region in successive layers.
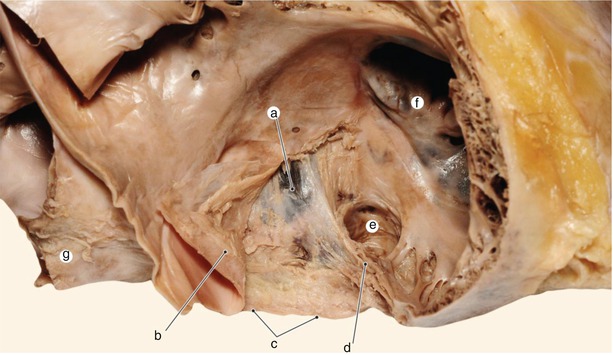
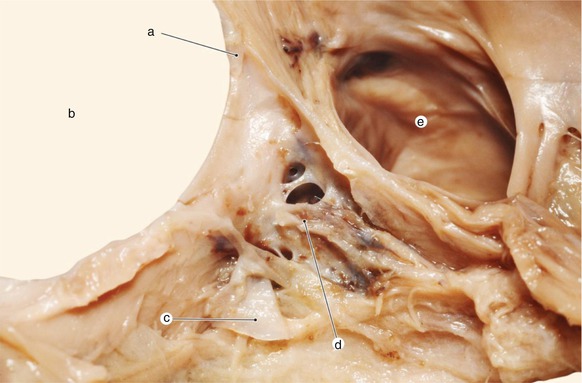
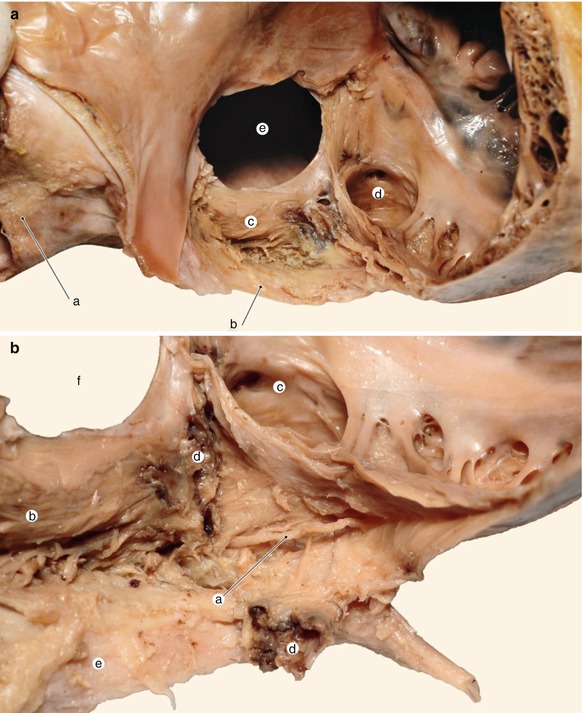
Fig. 6.33
Below the subendocardium muscle fibers we notice the reminiscences of the left valve which strengthen the floor of the fossa ovalis. The marginal fold is very well defined. a fossa ovalis, b endocardium and muscle fibers, c inferior vena cava, d eustachian edge, e Sinus ostium, f septal cusp of tricuspid valve, g right pulmonary veins
Fig. 6.34
Cavernous vascular structure in the depth of the dorsosinusal space. a primitive sinus valve commissure on the former septum secundum, b fossa ovalis, c left valve reminiscence, d cavernous vascular organ, e sinus ostium
Fig. 6.35
(a) The muscular fascicle in the depth of the dorsosinusal space could reprezent an interatrial connection path for the electrical impulse. a inferior right pulmonary vein, b inferior vena cava, c profound muscular fascicle in continuation of the muscular fibres surrounding the pulmonary vein, d sinus ostium, e fossa ovalis. (b) A nerve trunk accompanies the sinus in the depth of dorsosinusal space. a nerve trunk, b deep muscular fascicle, c sinus ostium, d the place where the cavernous organ was resected, e inferior vena cava, f fossa ovalis
In this area there are muscular fibers in the subendocardial space, which continue the ones in the limbus of the oval fossa and the muscular Eustachian margin.
Under these muscle fibers, the left valve of the embryonic venous sinus has fused with the septum primum and septum secundum during the embryological period.
For this fusion to be possible, the left valve has attached itself over (probably) the vestigial part of the right umbilical vein (found as a cavernous vascular structure) and then over the terminal segment of the coronary sinus (vestigial part of the left horn of the venous sinus) (Figs. 6.33 and 6.34).
Before merging with to the septum primum, a coalescent process has taken place the septoalveolar recess (the space found in the first stages of cardiac development between the interatrial septum and the left valve of the embryonic venous sinus), which led to the disappearance of this recess.
Attaching itself to the septum primum, between the valve and the septum, a mesenchymal area of probable extracardiac origin was included, area known as the dorsal mesenchymal protrusion.
This mesenchymal segment suffers a muscular transformation, resulting in deep muscle fascicles which complete the limbus of the oval fossa on at its inferior side (fascicles related to the muscles of the pulmonary veins) (Fig. 6.35).
! These muscular fascicles can represent an additional pathway for conduction.
Deep in the dorsosinusal space, under all these successive structures, the sinus wall can be observed, and parallel to it the nervous fibers from the cardiac plexus (Figs. 6.36 and 6.37).
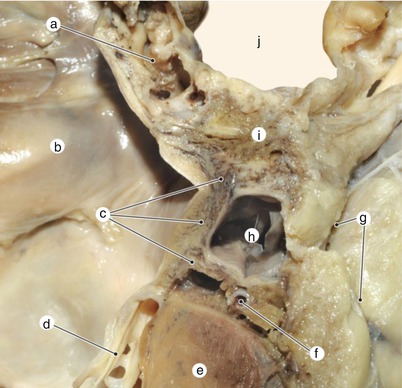

Fig. 6.36
Frontal section through the dorsosinusal space. View from the rear. Atrial septum does not reach the base of the ventricle. a cavernous organ, b left atrium, c perisinusal muscular fibers which continue the left atrium fibers, d posterior mitral cusp, e interventricular septum, f atrioventricular node artery in the pyramidal space, g epicardium, h coronary sinus, i dorsal sinus space, j right atrium
Fig. 6.37
Structural deficiency of the dorsosinusal space. View of the fossa ovalis from the right side. SVC superior vena cava, a limbus of fossa ovalis, b the floor of fossa ovalis, c structural deficiency of the dorsosinusal space due to lack of fusion of the left valve, d coronary sinus ostium, e eustachian edge, f septal cusp, g foramina
Review: in the structure of the dorsosinusal space from the luminal surface towards the deep surfaces we can find :
Endocardium
The subendocardial muscular layer
The vestigial part of the left valve which covers the reminiscent septovalvular recess
The vestigial part of the right umbilical vein (embryonic vascular-cavernous vestigial parts)
The muscularization of the dorsal mesenchymal protrusion
The sealing of the terminal segment of the coronary sinus (embedded in the atrium wall – chronologic stage in division).
We have made this journey in the embryogenesis of the area for understanding that the completion of atrial division is made through the consolidation of the posterior inferior part of the oval fossa and the dorsosinusal space!
Damage to this consolidation leads to inferior interatrialseptal defects of a venous sinus type.
The protrusion of the extraembryonic mesenchyme from the dorsal mesocardium in the atrium wall is a relatively new embryological term (also see embryology).
The consolidation of the septum necessarily requires the protrusion of the extraembryonic mesenchyme, the fusion of the left valve to the septum primum, the coalescence of the septoalveolar recess as well as the formation of the posterior limbus of the septum secundum through the folding of the right atrium wall. Failure of any of these stages is followed by a specific type of interatrial defect.
For a long period of time, the importance of the dorsosinusal space for the anatomy, electrophysiology and clinical study of the heart has been underestimated. Alongside with the evolution of electrophysiological studies and development of the capacity to block reentry mechanisms, the clinical significance of this area has been reconsidered.
! The vascular cavernous structure from the depth of the dorsosinusal space has not been described until now in scientific literature. The caverns certainly communicate with the venous blood flow. This structure could have its own pathology (inflammation or thrombosis).
6.1.4 The Tricuspid Vestibule
The tricuspid vestibule is a segment of the atrial cavity that originates in the embryonic atrioventricular canal. It is represented by a circular area with smooth walls that surrounds the opening of the tricuspid valve (Fig. 6.38).
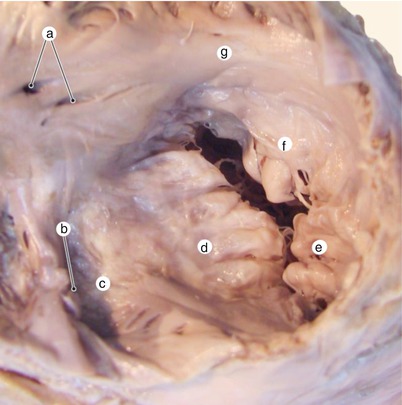
Fig. 6.38
Superior view of the tricuspid valve and tricuspid vestibule. a foramina, b coronary sinus ostium, c atrial floor, d septal cusp, e posterior cusp, f anterior cusp, g subauricular vestibule
The vestibule can be divided into several territories. The names of these territories are disputed and they are not adopted neither by the anatomical schools nor by nomina anatomica. We shall define these terms in the way that they are used in clinical anatomy.
These terms are: the atrial floor, the cavotricuspid isthmus, the subeustachian and thebesian sinuses, the Koch triangle, the subauricular part of the tricuspid vestibule.
6.1.5 The Floor of the Right Atrium
The floor of the right atrium is difficult to guess because the atrium is configured superiorly to the ventricle in many descriptions or representations. In these representations, the atrium has a floor located behind the tricuspid opening. In reality, the right atrium is located more to the posterior than superior to the right atrioventricular opening and the plane of the tricuspid opening is located on the anterior wall of the atrium. The term of “floor” is still kept and it refers mainly to the part of the atrial wall located between the attachment of the septal cusp, the eustachian border and the base of the interatrial septum (Figs. 6.39 and 6.40).
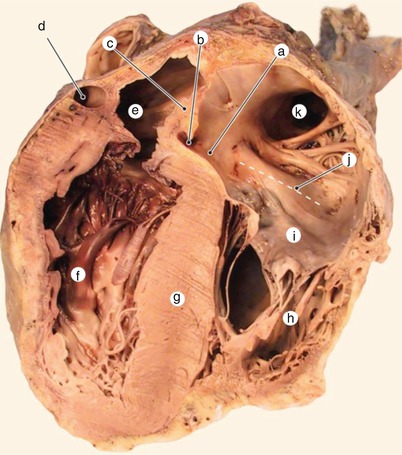
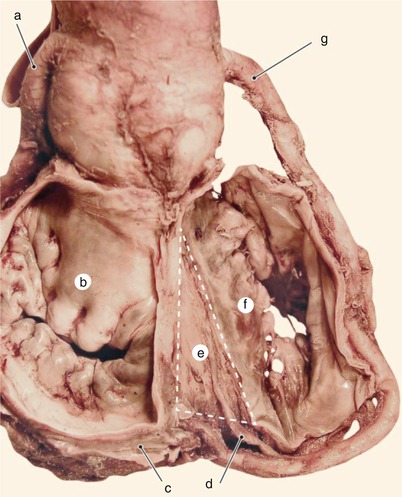
Fig. 6.39
Oblique section highlighting the four cavities. Posterior view. a atrial floor, b coronary sinus ostium, c interatrial septum, d coronary sinus, e left atrium, f left ventricle, g interventricular septum, h right ventricle, i anterior cusp, j subauricular vestibule, k right auricle
Fig. 6.40
After removal of the atria, the projection of the pyramidal space on the base of the interventricular muscular septum is highlighted. Superior and posterior view. a left coronary, b anterior cusp, c coronary venous sinus, d atrioventricular node artery, e floor of the pyramidal space, f septal cusp, g right coronary
The ostium of the coronary sinus represents the opening of the biggest vein of the heart in the floor of the right atrium. It is bordered posteromedially by a muscular fold that originates from sinus septi and by the eustachian border. This muscular fold is often mistaken for the ostial valve. The valve is an endocardic fold that borders variably (medially or laterally) the ostium of the coronary sinus and it originates from the right valve of the primitive venous sinus. It can sometimes be absent or can have exaggerated dimensions (exuberant) (Figs. 6.41, 6.42 and 6.43).
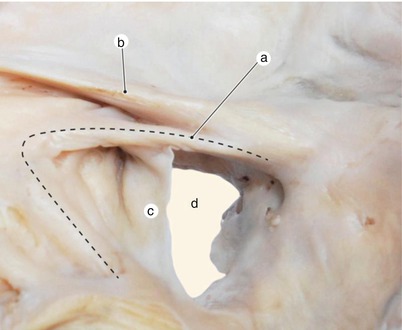
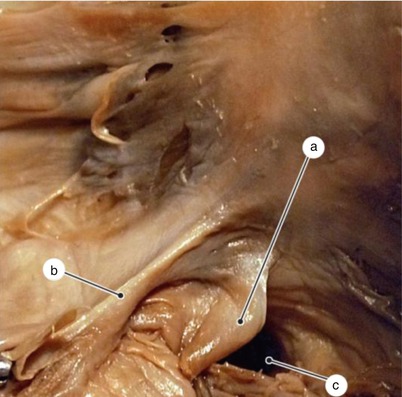
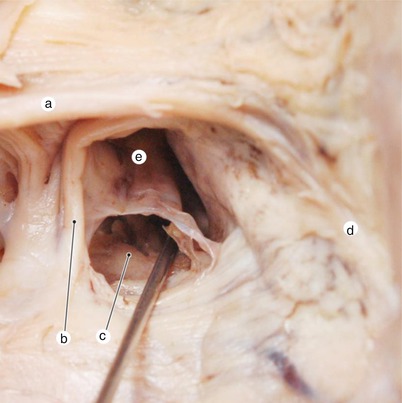
Fig. 6.41
Detail of the coronary sinus ostium, with explicit periosteal structures. a muscular edge from sinus septi, b Eustachian edge originating from the marginal fold, c Sinus valve originating from the right valve, d Coronary sinus ostium
Fig. 6.42
An exuberant valve of the sinus ostium can make more difficult the catheterisation procedure. a exuberant valve sinus, b eustachian edge, c coronary sinus ostium
Fig. 6.43
When the medium vein is draining into the right atrium at the level of the sinus ostium, sinus catheterisation can be missed. a eustachian edge arising from marginal fold, b muscular edge arising from sinus septi, c medium vein ostium, d todaro tendon, e coronary sinus ostium
The terminal crest unfolds inferiorly its muscular fibers like a fan, in a thin subendocardic layer.
These longitudinal subendocardic fibers reach the atrioventricular node forming the atrial floor (see excitoconductor system).
This thin subendocardic muscular layer is separated from the crest of the interventricular septum and the base of the right ventricle by a layer of connective-adipose tissue which continues the subepicardic adipose tissue from the crux cordis. The connective-adipose lamina enters between the right atrium and ventricle below and around the terminal segment of the coronary sinus.
The artery of the node, the veins and the nervous fibers reach the atrioventricular node through this connective-adipose lamina.
The space occupied by this connective-adipose lamina, located in the fold between the atrial wall and the base of the ventricle is called the pyramidal space (Fig. 6.36).
The performance of ablation procedures on the atrial wall presents the risk of injuring the nodal artery that crosses through this space either from the right coronary artery or from the left one.
In conclusion, if we insert a needle through the floor of the right atrium we first reach the pyramidal space, located extra cardially, and then enter the base of the right ventricle.
The division of the heart is not a process that results in symmetric chambers. While the vestibule of the left atrium is relatively symmetric, in the right atrium the vestibule is asymmetric. The floor of the right atrium coats a part of the base of the right ventricle and a part of the posterior segment of the crest of the interventricular septum (Fig. 6.39).
To have a correct image we remind you that the two atrioventricular rings are connected through the right fibrous triangle (the tendinous center). This triangle is located towards the left of the interventricular septum – it literally “floats” in the vestibule of the aorta (see the fibrous skeleton). The right triangle is a landmark for the base of the interatrial septum. We understand now that according to the width of the crest of the interventricular septum, the interatrial septum is moved towards the left and the floor of the right atrium lines the crest of the interventricular septum and the base of the right ventricle.
The left horn of the valve of the inferior vena cava is sometimes continued on the floor of the right atrium by the valve of the coronary sinus (these valves have a common embriological origin in the valve of the primitive venous sinus). In other cases, it is continued by the anterior extremity of the limbus of the fossa ovalis (this is also normal because at this level – of the septum secundum- the two valves of the primitive venous sinus have a merging area) (Figs. 2.48, 2.49 and 2.50).
6.1.5.1 The Spetal Isthmus and Cavotricuspid Isthmus
The septal isthmus is located on the floor of the right atrium, at the root of the interatrial septum, between the border of the coronary sinus and the insertion of the septal cusp. In the anatomical position of the heart, it is located superiorly to the cavotricuspid isthmus, for that being called the superior isthmus (Fig. 6.44).
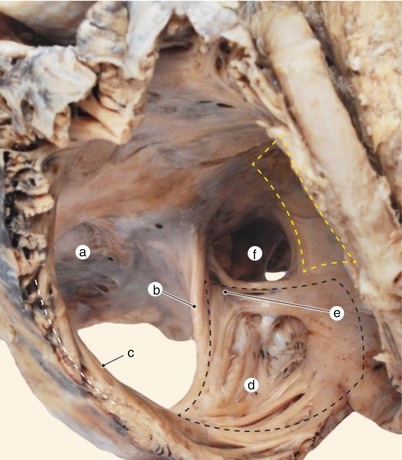
Fig. 6.44
Right atrium after the resection of the primitive wall. The position of the septal isthmus (yellow line) and the venous-tricuspid isthmus (black line). a fossa ovalis, b eustachian edge, c terminal crest, d subeustachian sinus, e subthebesian sinus, f coronary sinus ostium
This isthmus is crossed by the nervous impulse that follows the “slow path” in it’s way towards the atrioventricular node [1].
The cavotricuspid isthmus occupies most of the atrial floor.
It is bordered by the eustachian border and valve posteriorly and by the insertion of the septal cusp anteriorly; by the thebesian valve superiorly and inferiorly by a line that connects the opening of the vena cava with the insertion of the tricuspid valve.
It is also called the inferior isthmus, in order to be differentiated from the septal isthmus, located superiorly (Fig. 6.45).
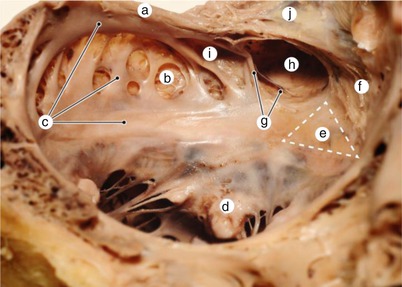
Fig. 6.45
Venous-tricuspid isthmus and vestibular topography. Anterior view. a eustachian edge, b subeustachian sinus, c venous-tricuspid isthmus (trabecular, central and anterior parts), d septal cusp, e Koch triangle, f septal isthmus, g thebesian valve, h sinusal ostium, i subthebesian sinus, j dorsosinusal space
The cavotricuspid isthmus is a major part of the circuit responsible for most types of flutter [2].
The cavotricuspid (or inferior) isthmus has three parts:
The trabeculated part, represented by the eustachian border. It is also called the posterior sector. Its structure consists of a fibro-adipose component and muscular fibers (see the formation of the eustachian border).
The central part, membranous, represented by the two subeustachian and subthebesian recesses (or the Keith sinus). Here its aspect is characterized by the presence of some muscular trabeculae that divide very thin membranous segments.
The anterior part, vestibular, located in the vicinity of the insertion of the septal cusp. This part is smooth, nontrabeculated, its wall being formed entirely by thin atrial miocardium. The myocardial fibers that emerge from the terminal crest are generally parallel and lead towards the Koch triangle. However, in the vicinity of the sinusal opening there are still some crossings of muscular fibers.
6.1.5.2 The Tendon of Todaro
The tendon of Todaro is a fibrous subendocardic, inconstant cord, with variable development and aspect. It is about 0.5–1.5 cm long and 1–2 mm thick. Most frequently, after cutting and removing the endocardium, it appears as a thin connective cord, bright white, resembling a tendinous cord. Its insertion is on the right triangle, above the atrioventricular node. Its origin fades at the level of the left horn of the Eustachian valve, in the dorsosinusal space.
The tendon of Todaro may have a fibro-cartilaginous appearance. It is sometimes replaced by a muscular trabecula that extends from the limbus of the fossa ovale, taking the name of the tendon of Todaro (Figs. 6.46, 6.47 and 6.48).
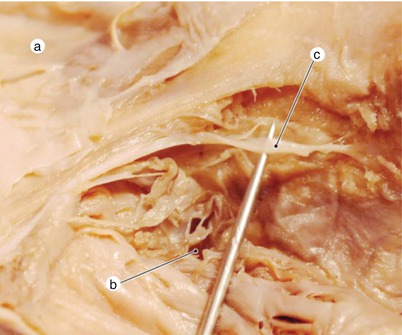
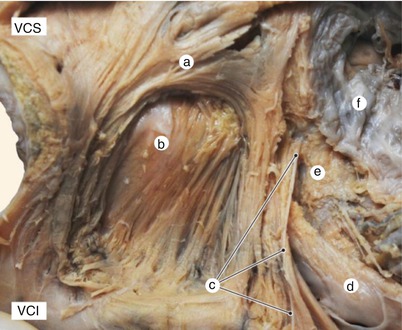
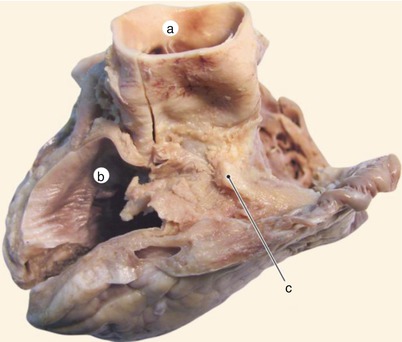
Fig. 6.46
Highlighting the tendon of Todaro. a dorsosinusal space, b coronary sinus ostium, c tendon of Todaro
Fig. 6.47
The tendon of Todaro begins in the dorsosinusal space and inserts in the tendinous center, superior to the atrioventricular node. Posterior and lateral view. a limbic fascicle, b the floor of the muscled fossa ovalis, c todaro tendon, d coronary sinus ostium, e atrioventricular node, f septal cusp
Fig. 6.48
Base of the ventricular pyramid after removing the atria. a aorta, b left atrium, c tendon of Todaro turned cartilaginous
6.1.5.3 The Koch Triangle
The need for some topographical guidance for the location of the atrioventricular node led to the definition of the Koch triangle.
This is located in the left extremity of the floor of the atrium, in the angle between the base of the septum and the insertion of the septal cusp.
When subendocardially we can find and palpate the tendon of Todaro at the base of the interatrial septum, the region is called the Koch triangle. This region actually corresponds mostly to the superior isthmus.
The atrioventricular node is located in the anterior and superior angle of the triangle.
Underneath the endocardium of this region there can be found the artery of the atrioventricular node, coming from the crux cordis or from the right coronary groove.
The triangle has the following borders:
Anteriorly and to the left, at the apex of the triangle, by the right fibrous triangle and the membranous septum. The fibrous triangle can be felt endocardially. It is crossed by the perforating part of the Hiss bundle.
The left border is formed anteriorly by the tendon of Todaro (subendocardic and intramuscular) and posteriorly by the ostium of the coronary sinus.
The right border is an imaginary line that continues anteriorly the right part of the ostium of the coronary sinus, up to the intersection with the insertion of the septal cusp.
The anterior border is the insertion line of the septal cusp, up to the right fibrous trigone (Figs. 6.49).
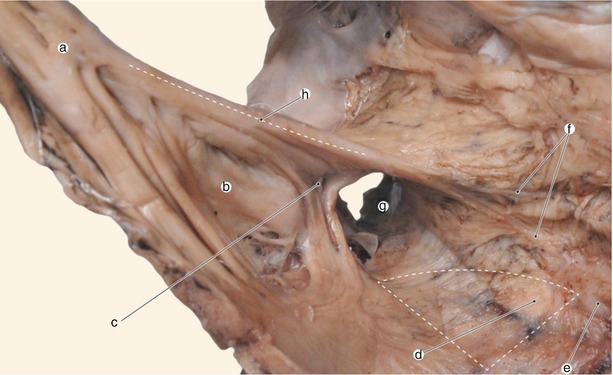
Fig. 6.49
The position of the atrioventricular node. Anterior view. a terminal crest whose inferior extremity splits, b subeustachian sinus, c subthebesian sinus, d atrioventricular node, e atrioventricular septum, f bifurcated Todaro tendon, g coronary sinus ostium, h eustachian edge
In the area of the triangle, at the tip, there lies the atrioventricular node. More precisely, the node is located at the base of the right ventricle, bordered by the right fibrous triangle, contained partially in the connective-adipose lamina between the floor of the right atrium and the base of the right ventricle (at the tip of the pyramidal space).
! The quick definition of the triangle can be made as follows: in the right atrium, the floor has a flat region located between the origin of the septal cusp, the ostium of the venous sinus and the base of the interatrial septum. The left and superior extremity of this region is the Koch triangle.
6.1.5.4 The Terminal Crest
The terminal crest is a muscular semicircular prominence that separates the atrial territory derived from the primitive atrium from the atrial territory derived from the venous sinus. On the outer surface it corresponds to a shallow groove called the sulcus terminalis. It derives from the fusion of the terminal fasciculus and the marginal fold (see embryology).
The terminal crest describes an almost circular course, beginning and ending in contact with the interatrial septum and it splits the right atrium embryologically, morphologically and functionally Figs. 6.12, 6.49, 6.50 and 6.51).
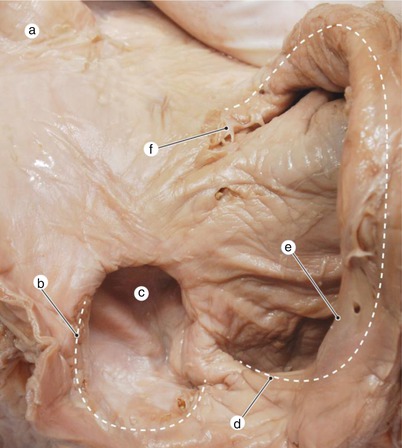
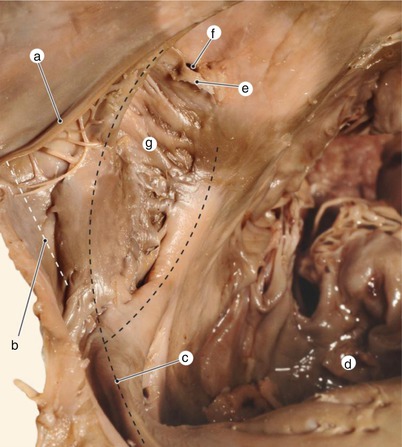
Fig. 6.50
Right atrium from the right and rear view. The atrial wall was folded over the terminal crest so the general disposition of the terminal crest can be highlighted. Valvular reminiscences (marked with dotted lines) demonstrate the initial disposition of the primitive sinus valves. a superior vena cava, b left valve reminiscence, c interatrial patent orifice, d right valve reminiscence, e inferior vena cava valve, f right valve reminiscence (named by some “superior vena cava valve”)
Fig. 6.51
Due to a deficienty of coalescence of the right valve, in an adult heart a rest of venous-marginal recess can be noticed. The existence of the superior bifurcation fascicle of the terminal crest explains the possibility of impulse conduction through the trabeculated part of the venous-tricuspid isthmus. View from the right and superior. a valve of the inferior vena cava, b venous-marginal recess with incomplete coalescence, c terminal crest which bifurcates inferiorly, d posterior cusp, e thebesian valve, f sinusal ostium, g subeustachian sinus
The terminal crest begins superiorly at the right of the opening of the superior vena cava (it is here in relative continuity with a sagitaltrabecula inside the right auriculus) (Fig. 6.9). It then descends on the anterior-lateral wall of the atrium. On this wall it gives two types of muscular trabeculae:
one group of almost vertical ascending trabeculae, located in the upper part of the crest, difficult to spot and to demonstrate, that lie between the atrial crest and the atrial wall. These muscular cords are thin and they are usually continued by the subepicardic muscle fibers (Fig. 6.10).
The pectinate muscles also enter the right auriculus. The pectinate muscles sometimes attach on the sagital trabecula following a pattern that resembles the fibers of a palm-tree leaf (Fig. 6.52). Other times, the distribution of the pectinate muscles is “palmed” (Fig. 6.6).
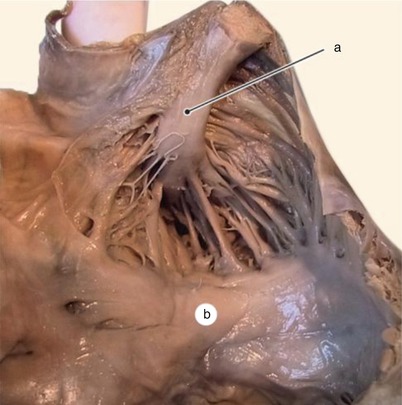
Fig. 6.52
Variant of distribution of the pectinate muscles in the right auricle. a sagittal trabeculae in the axis of the right auricle, b subauricular vestibule
The atrial wall between the pectinate muscles is very thin, having a membranous aspect.
The behavior of the terminal crest towards the atrial floor is inconstant. It generally divides into two muscular fascicles, with a variable aspect (Figs. 6.49 and 6.51), called the posterior and anterior fascicles.
The posterior fascicle lines the valve of the inferior vena cava (Eustachio), forming together the eustachian border.
In intrauterine developement there is a cavomarginal recess1 (proposed term) between the right valve of the embryonary venous sinus and the marginal fold.
This recess disappears through a coalescence process so that in the adult the Eustachian valve adheres to the terminal crest. Some rudimentary chordae may remain as imperfections of this coalescence (Fig. 6.51).
The anterior fascicle heads towards the septal cusp, some of its fibers diverging as a fan in the subendocardic layer of the floor of the atrium.
The muscle fibers of both fascicles reach the atrioventricular node.
There is a so-called “subeustachian” recess that generally has few muscular trabeculae. The atrial wall in this region is thin, membranous. Towards the left side of the subeustachian recess, in connection with the ostium of the coronary sinus there is a smaller recess, called the subthebesian recess (the sinus of Keith) (Fig. 6.49).
The right horn of the valve of the inferior vena cava is sometimes continued upwards by remnants of the right valve of the embryonary venous sinus. They reach the right side of the opening of the inferior vena cava as small membranes or tendinous chordae sometimes being excessively considered as proof of existence of a valve of the superior vena cava (Fig. 6.50).
6.1.5.5 The Subauricular Part of the Vestibule of the Right Atrium
The subauricular part of the vestibule is the segment of the vestibule located anteriorly and superiorly, between the base of the right auricle and the tricuspid ring. It is embryologically derived from the incorporation in the atrial wall of a part of the right atrioventricular junction (Fig. 2.80).
This part corresponds on the exterior to the right anterior segment of the coronary groove. The openings of some thebesian veins can be seen here.
The anterior veins of the right atrium and ventricle sometime open in a deep venous channel located in the thickness of the vestibular wall. This channel has an entrance bordered by an endocardic semilunar fold (sometimes the entrance is covered by pectinate muscles). The length and diameter of the channel vary, the maximal dimensions being 2.6/0.6 cm (Figs. 6.53 and 6.54).
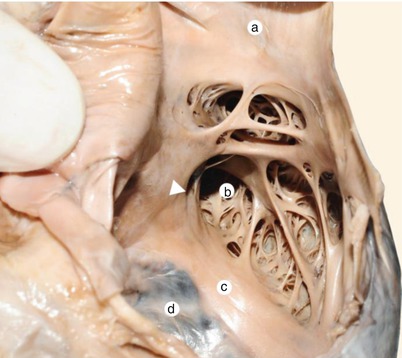
Fig. 6.53




Demonstration of the subaricular vestibule in the right atrium. The arrowhead indicates the drainage orifice of a deep venous canal. a superior vena cava, b right auricle, c subauricular vestibule, d anterior cusp
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
