Innocent Murmurs
“One needs to know what is normal before one can know what is abnormal”
Most children, at some time, will have a heart murmur. However, very few of these children will have heart disease. The physician’s task is to determine whether the murmur is the result of a cardiac abnormality or is a so-called innocent or functional murmur.
Although an innocent murmur is not an obstacle to participation in sports and exercise, a pathologic murmur may necessitate restrictions on the child’s physical activity. In view of the safety considerations and the importance of exercise and fitness, it is crucial to resolve any doubt about the nature of a murmur.
Innocent murmurs occur in all age-groups in the absence of structural heart disease. Their quality and intensity depend upon environmental conditions and the subject’s state. For example, conditions that increase cardiac output, such as fever, anxiety, and exercise, will make an innocent murmur louder. The examiner’s ability to hear a murmur depends on the presence of distracting ambient noise, patient cooperation, the examiner’s hearing acuity, the quality of the stethoscope, and the thickness of the patient’s chest wall.
The diagnosis of an innocent murmur is not made by exclusion, but rather is based on physical findings that indicate that the specific murmur is innocent. There are five innocent murmurs of infancy and childhood: (i) pulmonary flow murmur, (ii) Still’s murmur, (iii) venous hum, (iv) carotid bruit, and (v) physiologic pulmonary branch stenosis of the neonate (see Figs. 5.1 and 5.2). All these murmurs usually are between 1 and 2 out of 6 on the intensity scale, and all feature normal first and second heart sounds, peripheral pulses, and precordial impulses.
Pulmonary Flow Murmur
Pulmonary flow murmur results from turbulent blood flow through an anatomically normal pulmonary valve. It probably is the most common innocent murmur of childhood and is more often heard in children and adolescents than in adults because of the relatively faster blood flow and thinner chest wall of young patients. Pregnant women often will have a pulmonary flow murmur because of the relatively hyperkinetic circulation and increased plasma volume during pregnancy.
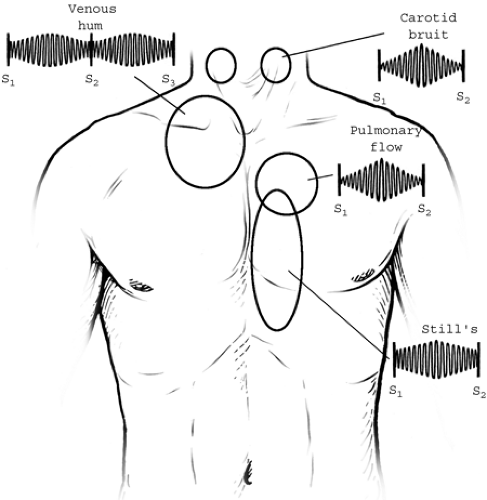 Figure 5.1 • Location and characterization of four of the five innocent murmurs of childhood. |
 Figure 5.2 • Illustration of the basis of physiologic pulmonary branch stenosis of the newborn. The murmur is similar to the innocent pulmonary flow murmur. It is heard best at the upper left sternal border and heard well in the axillae and over the back. |
An innocent pulmonary flow murmur is best heard at the mid and left upper sternal border. It is a midfrequency, crescendo–decrescendo sound that occurs during systole. The murmur is louder with the patient in the supine rather than the upright position. The normal second heart sound distinguishes an innocent pulmonary flow murmur from that of an atrial septal defect, in which the second heart sound is widely split and relatively fixed during the respiratory cycle. The “right ventricular impulse” palpated at the lower left sternal border or subxiphoid area is normal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


