The remarks of Paul Ridker, MD, in the recent “Editor’s Roundtable” require comment. Ridker declares high-sensitivity C-reactive protein (hsCRP) to be a major risk factor for atherothrombotic disease (ATD). Dr. Ridker is in error in this statement. If hsCRP were a major ATD risk factor, then subjects with the highest levels of hsCRP should have the highest risk for ATD, and as Ridker himself has pointed out, natives of sub-Saharan Africa frequently have malaria, and those who do have malaria have extremely high levels of hsCRP but do not have ATD events to any significant degree. This finding is consistent with Dr. Roberts’s observation that patients with rheumatoid arthritis and systemic lupus erythematosus have only a slight increase in atherosclerotic plaque. Moreover, it is common knowledge, as confirmed by Dr. Friedewald, that nonsteroidal agents are excellent anti-inflammatory agents but actually increase the risk for ATD events. Finally, many conditions other than ATD cause increases in hsCRP, which is why repetitive testing is necessary to confirm the initial hsCRP result. Hence, hsCRP cannot be a major risk factor for ATD: risk factors actually cause ATD, but, in contrast, markers of ATD simply denote the presence of ATD. Indeed, Ridker pointed out in the early days of hsCRP that it is a marker for the inflammatory response to known ATD risk factors: cigarette smoking, dyslipidemia, and hypertension, and I might even add diabetes mellitus to this list.
Dr. Ridker also states that a low-density lipoprotein (LDL) level of <130 mg/dl is low. The average LDL at which an ATD event occurs in Wood County, Ohio, is 145 mg/dl in men and 154 mg/dl in women; thus, an LDL in the range of 130 mg/dl is not that low. The population at risk for ATD is easily and accurately predictable by a global risk factor graph, but only when a ratio between LDL and high-density lipoprotein (HDL) is used (such as the cholesterol retention fraction, defined as LDL-HDL/LDL). If only LDL is used, the accuracy of the predictive graph decreases dramatically (Feeman, unpublished data). This finding is illustrated by the case report of Dr. Davidson: a woman with a strong family history of ATD, LDL of 100 mg/dl, high-density lipoprotein of 20 mg/dl, and hsCRP of 6 mg/L. Her LDL probably would not usually be considered for treatment, but her cholesterol retention fraction is 0.80, which is in the highest sextile and warrants therapy. In my experience, however, ATD events in patients with this type of dyslipidemia, in the absence of cigarette smoking, do not happen until very late in life, unless these lipids have been present since birth. (Incidentally, an hsCRP value of 6 mg/L is high enough to suggest a non-ATD origin.)
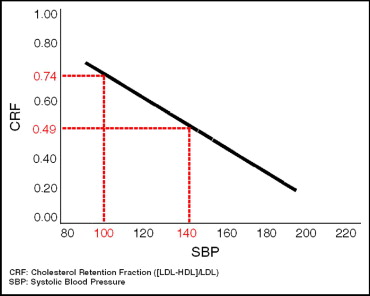
The global risk factor graph has been presented in The American Journal of Cardiology , and I include it in this comment for illustrative purposes ( Figure 1 ) . The line determinants are based on lipid values obtained when HDL is measured by the indirect technique; if HDL is measured by the direct technique, then the line co-ordinates are (0.62, 100) and (0.40, 140).