Increasing Shortness of Breath
A 25-year-old medical student had a 6-month history of increasing shortness of breath. Since childhood, he was less physically fit than his classmates, but this was always attributed to his obesity (body mass index of 32). He had no medical history of cardiac disease. A transthoracic echocardiogram was performed, revealing aortic stenosis with a mean gradient of 42 mm Hg and mild aortic regurgitation.
For a more detailed assessment of the aortic valve, a transesophageal echocardiogram (TEE) was performed (Figs. 4-1, 4-2, 4-3, 4-4 and 4-5).
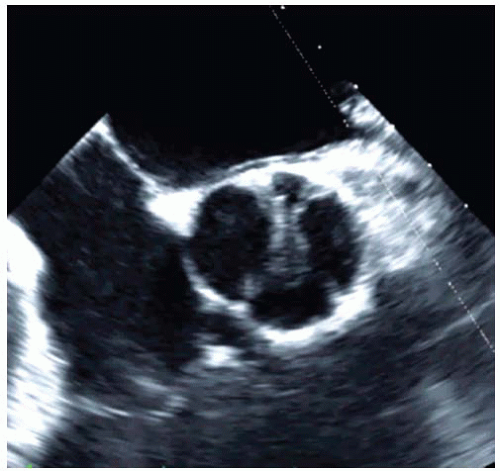 Figure 4-1. 2D TEE: Midesophageal short-axis view (60°) of the aortic valve in diastole. |
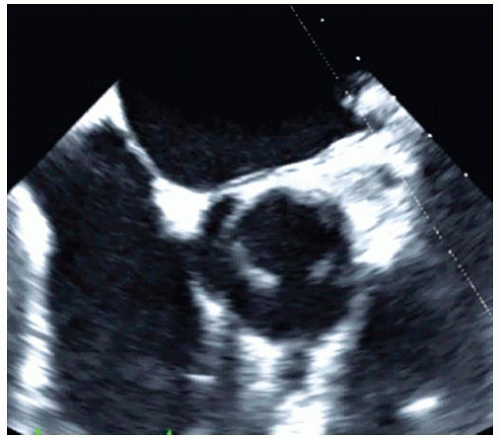 Figure 4-2. 2D TEE: Midesophageal short-axis view (60°) of the aortic valve in systole. |
 Figure 4-3. 3D TEE: Enface view of the aortic valve in diastole. |
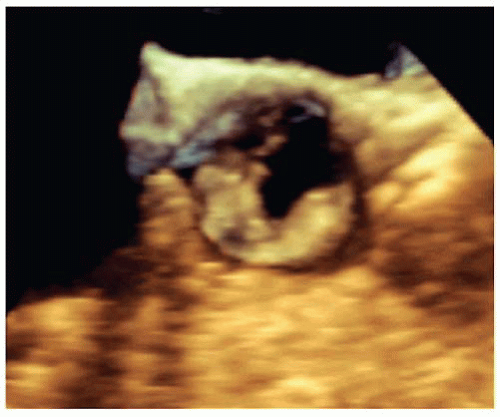 Figure 4-4. 3D TEE: Enface view of the aortic valve in systole. |
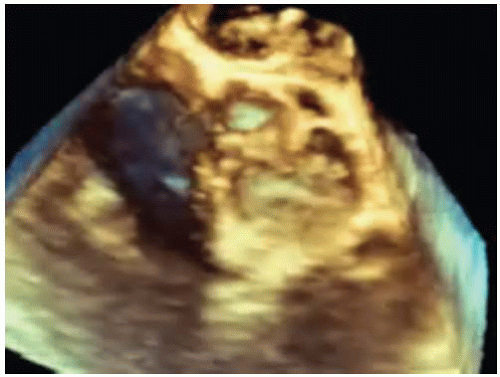 Figure 4-5. 3D TEE: Enface view of the aortic valve. |
QUESTION 1. What is his diagnosis?
A. Rheumatic aortic valve disease
B. Bicuspid aortic valve
C. Calcific disease of a trileaflet aortic valve
D. Unicommissural aortic valve
E. Acommissural aortic valve
View Answer




ANSWER 1: D. Isolated rheumatic aortic valve stenosis is a rare disease. There is no history of rheumatic fever in the patient’s history, and the aortic leaflets are not demonstrating the typical morphology for rheumatic heart disease with cusp thickening and commissural fusion. Therefore, this diagnosis is highly unlikely in this patient.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
