, Malissa J. Wood2 and Malissa J. Wood3
(1)
Harvard Medical School Cardiology Division, Department of Medicine, Massachusetts General Hospital, Boston, MA, USA
(2)
Harvard Medical School, Boston, MA, USA
(3)
MGH Heart Center Corrigan Women’s Heart Health Program, Cardiology Division, Department of Medicine, Massachusetts General Hospital, Boston, MA, USA
Abstract
To prepare for the imaging studies section of the board exam, you MUST know the answer option lists for the section INSIDE AND OUT. You can find the answer option lists on the American Board of Internal Medicine (ABIM) official website, http://www.abim.org/, under the tab, “take the exam your complete guide,” then under the “Prepare for the Exam: Take the Tutorial” section, near the bottom is a pdf file called “Sample Cases – Electrocardiograms and Imaging Studies (pdf).” Pay extra attention to the last page, which explains the scoring of sample cases.
Abbreviations
A3C
Apical 3 chamber or apical long axis
A4C
Apical 4 chamber
A5C
Apical 5 chamber
Ao
Aorta
ASD
Atrial septal defect
AV
Aortic valve
CW
Continuous wave
DT
Deceleration time
Ef
Effusion
HOCM
Hypertrophic obstructive cardiomyopathy
LA
Left atrium
LAD
Left anterior descending artery
LAO
Left anterior oblique
LCx
Left circumflex coronary artery
LIMA
Left internal mammary artery
LM
Left main coronary artery
LV
Left ventricle
LVOT
Left Ventricular outflow track
MR
Mitral regurgitation
MV
Mitral valve
OM
Obtuse marginal
PA
Pulmonary artery
PFO
Patent foramen ovale
PLAX
Parasternal long axis
PSAX
Parasternal short axis
Pulm
Pulmonary
PW
Pulsed wave
RA
Right atrium
RAO
Right anterior oblique
RCA
Right coronary artery
RPA
Right pulmonary artery
RV
Right ventricle
RVOT
Right ventricular outflow track
SAM
Systolic anterior motion
SVG
Saphenous vein graft
TEE
Transesophageal echo
ToF
Tetralogy of Fallot
TTE
Transthoracic echo
TV
Tricuspid valve
VSD
Ventricular septal defect
To prepare for the imaging studies section of the board exam, you MUST know the answer option lists for the section INSIDE AND OUT. You can find the answer option lists on the American Board of Internal Medicine (ABIM) official website, http://www.abim.org/, under the tab, “take the exam your complete guide,” then under the “Prepare for the Exam: Take the Tutorial” section, near the bottom is a pdf file called “Sample Cases – Electrocardiograms and Imaging Studies (pdf).” Pay extra attention to the last page, which explains the scoring of sample cases.
In this section, we have put heavy emphasis on the specific diagnoses that are on the answer option lists to complement bread and butter clinical training in imaging. We have included still-frame images with illustrate key findings, however, the actual exam contains moving images and will require COMPLETE CODING OF ALL YOU SEE RATHER THAN JUST THE KEY FINDINGS. All of the still-frame images in this chapter are available as moving images on our multi-media website. See Fig. 35-1 for an example of complete coding. The number of each key finding corresponds to the number of the diagnosis on the answer option sheet, but be mindful that the exact number may change over time as the answer option list evolves. We recommend that you try viewing the movies on the website with ABIM answer options list and code each and every case in a timed manner first.
Please note that ventriculograms and aortograms are no longer covered in the Imaging Studies section of the board. However, they will be continued to be covered under the multiple choice questions section and are briefly covered here.
Acknowledgements: We would like to acknowledge Dr. Michael Fifer for his assistance in selecting cardiac catheterization images.
Quick index with figure numbersEchocardiograms | 28. Patent ductus arteriosus |
1. Cardiac amyloidosis | 29. Patent foramen ovale |
2. Hypereosinophilic syndrome | 30. Primum atrial septum defect |
3. Noncompaction | 31. Secundum atrial septal defect |
4. Hypertrophic obstructive cardiomyopathy | 32. Membranous ventricular septal defect |
5. Takotsubo (stress induced) cardiomyopathy | 33. Tetralogy of Fallot |
6. Myocardial infarction | Angiograms |
7. LV apical aneurysm | 34. Ostial LM lesions |
8. LV pseudoaneurysm | 35. RCA lesion |
9. LV apical laminar thrombus | 36. Coronary thrombus and coronary dissection |
10. Intracardiac thrombus | 37. Coronary vasospasm and air embolism |
11. Pulmonary embolism | 38. Left-to-right collateral blood flow |
12. Tamponade | 39. Myocardial bridge and an LAD to PA fistula |
13. Mitral stenosis | 40. LCx arising from the right coronary cusp |
14. Flail anterior MV leaflet | 41. LCx arising from the RCA |
15. MV prolapse | 42. Venous bypass grafts |
16. Carcinoid | 43. Patent LIMA bypass graft |
17. Aortic valve, tri, bi, unicuspid | Ventriculograms and aortograms |
18. Calcific aortic stenosis | 44. Anterior aneurysm |
19. Aortic dissection | 45. LV pseudoaneurysm |
20. Coarctation of the aorta | 46. Dilated cardiomyopathy |
21. Mechanical AV dehiscence | 47. Takotsubo (stress) cardiomyopathy |
22. Mechanical mitral valve | 48. Severe mitral regurgitation |
23. Thrombus on a mechanical MV | 49. Aortic root abscess |
24. AV endocarditis | 50. Subclavian artery stenosis |
25. Atrial myxoma | |
26. Papillary fibroelastoma and lipomatous hypertrophy of the interatrial septum | |
27. Ebstein anomaly |
Echocardiograms
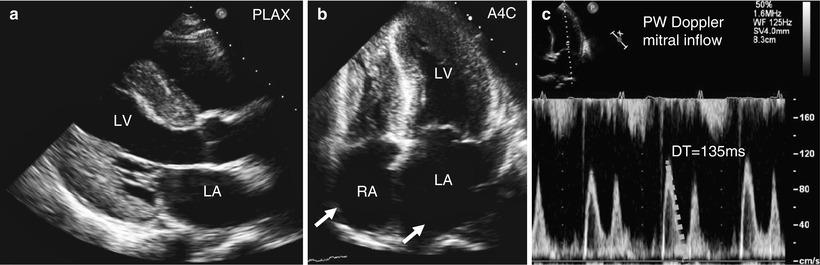
Fig. 35-1
A 47 year-old man with renal failure and syncope. Cardiac amyloidosis. 2D TTE images show biventricular hypertrophy, increased myocardial reflectivity, as well as biatrial enlargement (arrows) (a, b). Panel (c) showing PW Doppler at the mitral valve leaflet tips revealing a steep deceleration slope characteristic of a restrictive filling pattern. Key findings: 7. Grade 3 (restrictive) diastolic dysfunction, 16. Concentric LV wall thickness, 68. Enlarged left atrium, 69. Enlarged right atrium, 121. Amyloid. Complete coding: (in addition to above) 1. Normal LV size, 8. Normal WM, 12. Normal to hyperdynamic (≥50 %), 61. RV Normal size and function, 137. Pericardial effusion
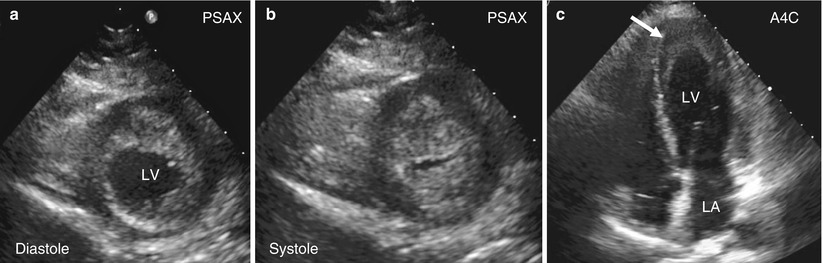
Fig. 35-2
A 45 year-old man with eczema and dyspnea. Hypereosinophilic syndrome. 2D TTE images showing PSAX in diastole (a) and systole (b) with significant LV soft tissue/eosinophils and thrombus deposition (arrow) at the apex of the heart (usually obliterating the apex), and no underlying wall motion abnormality. Panel (c) showing apical 4 chamber view of the same process. Make sure to be able to differentiate this from apical hypertrophic cardiomyopathy (which maintains a slitlike opening in the apex). Key findings: 19. LV mass or thrombus, 122. Hypereosinophilia
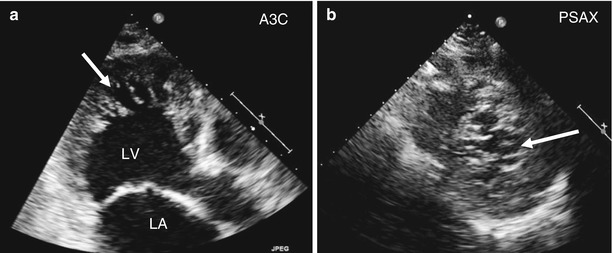
Fig. 35-3
A 35 year-old woman with stroke-like symptoms. LV Non-compaction. 2D TTE showing a thickened myocardium with a deeply trabeculated (arrow) appearance with intramyocardial sinusoids. Apical long axis (a) and PSAX (b) views are shown. Key findings: 119. Noncompaction
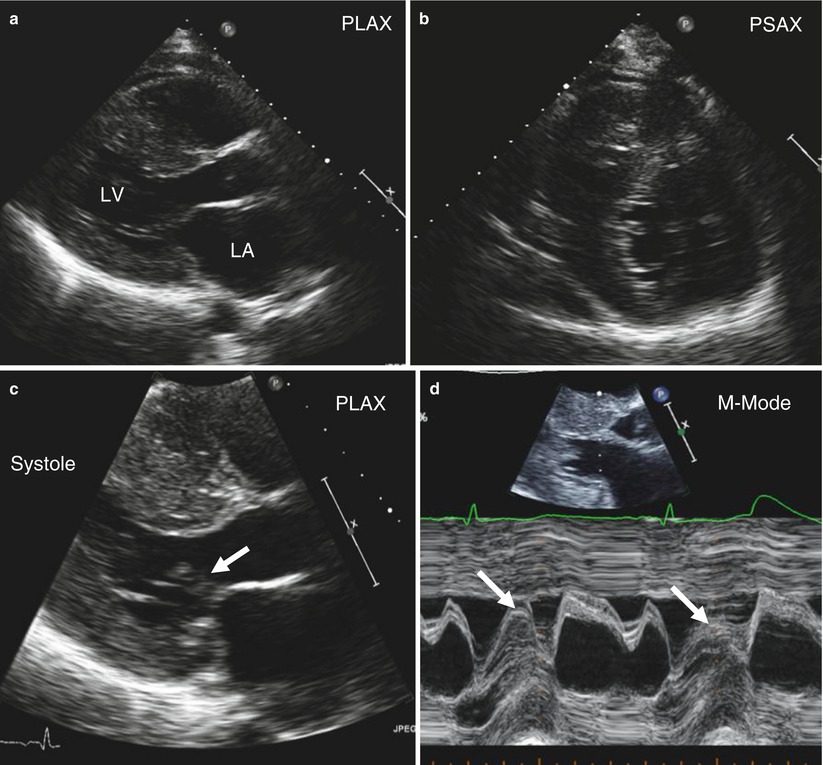
Fig. 35-4
A 45 year-old woman with syncope. HOCM. 2D TTE showing asymmetric septal hypertrophy in PLAX (a) and PSAX (b). Panel (c) showing SAM (arrows) also evident by MMODE in panel (d). Key findings: 17. Asymmetric septal hypertrophy, 18. LVOT obstruction/SAM, 114. Hypertrophic cardiomyopathy
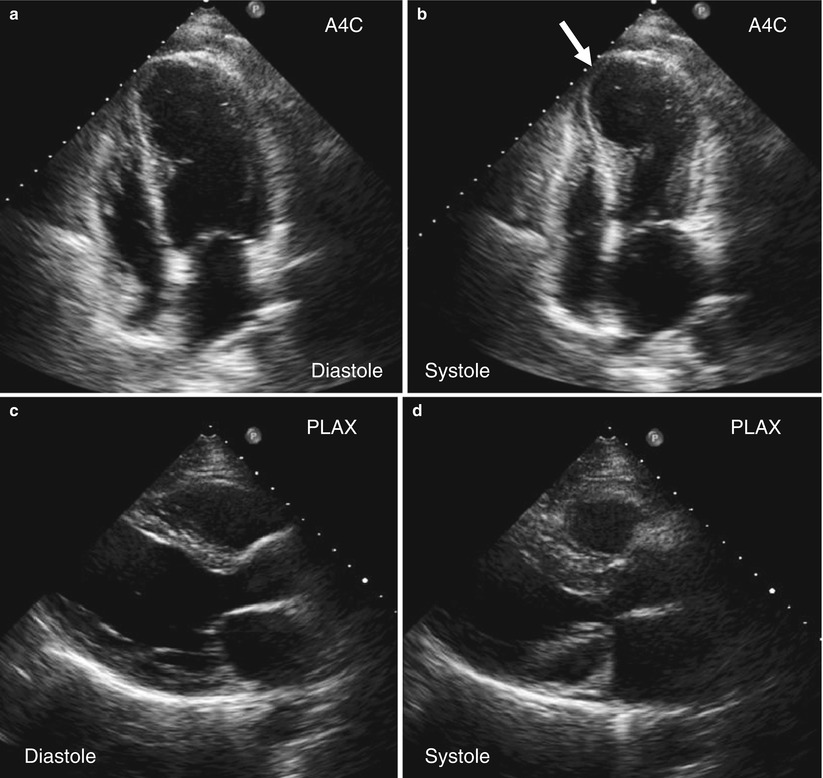
Fig. 35-5
A 77 year-old woman with chest pain at her husband’s funeral. Stress induced (Takotsubo’s) cardiomyopathy. 2D TTE showing an apical 4 chamber diastolic (a) and systolic (b) frames with apical hypokinesis (arrow) and preserved function at the base. PLAX diastolic (c) and systolic (d) frames are also shown. Key findings: 13. Mild to moderately reduced EF, 30. Apical hypokinesis, 120. Takotsubo (stress induced) cardiomyopathy
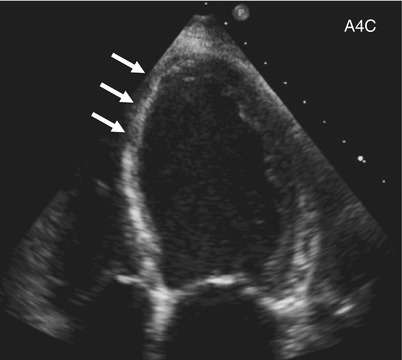
Fig. 35-6
A 65 year-old diabetic with crushing sub-sternal chest pain 1 year ago. Myocardial scar. 2D TTE apical 4 chamber showing a thinned and echo-bright septum (arrow) characteristic of scar formation. Key findings: 2. Enlarged LV size, 37. Septal thinning and/or scar
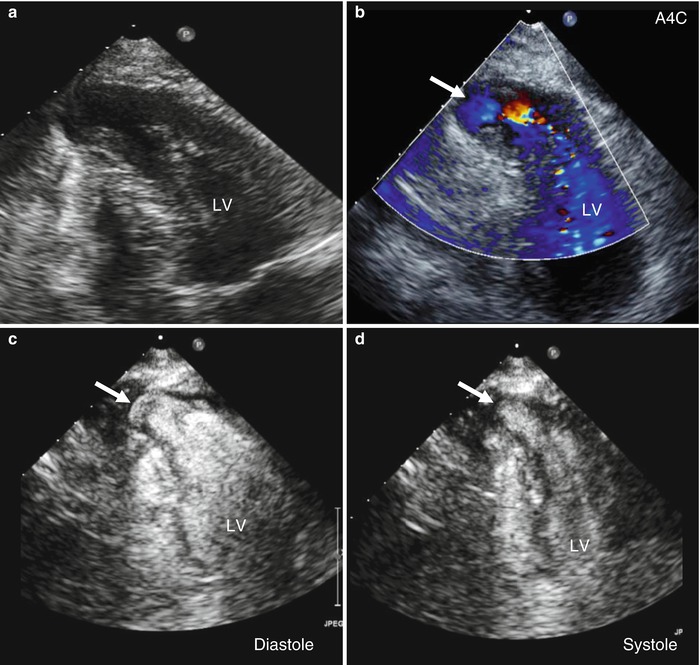
Fig. 35-7
A 76 year-old man with history of prior infarction. LV apical aneurysm. 2D TTE. Panel (a) shows an apical 4 chamber view of the aneurysm with color Doppler flow (b) into the aneurysm (arrow). Diastolic (c) and systolic (d) frames with LV contrast clearly show myocardial contraction in the aneurysmal segment (arrows). Key findings: 45. Apical aneurysm
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


