Subset of CAD by anatomy
Classa
For prognosis
Left main >50 %b
I
Any proximal LAD stenosis >50 %b
I
2VD or 3VD with impaired LV functionb
I
Proven large area of ischemia (>10 % of LV)
I
Single remaining patent vessel >50 % stenosisb
I
1VD without proximal LAD and without >10 % ischemia
III
For symptoms
Any stenosis >50 % with limiting angina or angina equivalent, unresponsive to OMT
I
Dyspnea/CHD and >10 % LV ischemia/viability supplied by >50 % stenotic artery
IIa
No limiting symptoms with OMT
III
Patients with persistent limiting symptoms (angina or angina equivalent) despite OMT for symptomatic benefit.
Certain anatomical patterns of disease (Table 8.1) or a proven significant ischemic territory even in asymptomatic patients for prognostic benefit. Significant LM stenosis and significant proximal LAD disease, especially in the presence of multivessel CAD, are strong indications for revascularization.
8.1.2 Indication for CABG Versus PCI in Stable CAD
CABG appears to be better in terms of survival benefit as well as reduction of revascularization in patients with high risk of CAD; multivessel disease with complex morphology and left main disease (Table 8.2) [2].
Table 8.2
Indications for CABG versus PCI in stable CAD patients
Subset of CAD by anatomy
Favors CABG
Favors PCI
Classa
Classa
1VD or 2VD – non-proximal LAD
IIb
I
1VD or 2VD – proximal LAD
I
IIa
3VD simple lesions, full-functional revascularization achievable with PCI, SYNTAX score ≤22
I
IIa
3VD complex lesions, incomplete revascularization achievable with PCI, SYNTAX score >22
I
III
Left main (isolated or 1VD, ostium/shaft)
I
IIa
Left main (isolated or 1VD, distal bifurcation)
I
IIb
Left main + 2VD or 3VD, SYNTAX score ≤32
I
IIb
Left main + 2VD or 3VD, SYNTAX score >32
I
III
8.2 Coronary Stent
8.2.1 Clinical Background
Coronary stents, which was developed in the mid-1980s, have been preferred method of performing PCI and replaced plain balloon angioplasty [3].
Drug-eluting stents (DES) are highly efficacious at reducing the risk of target-vessel revascularization without an increase in any safety outcomes, including stent thrombosis [4].
In contemporary PCI practice, newer-generation DES with novel coating and biodegradable stents are widely used.
Newer-generation DES have thinner stent struts for improvement of stent deliverability and more biocompatible polymers coating for reduction of in-stent restenosis (Fig. 8.1) (Table 8.3).
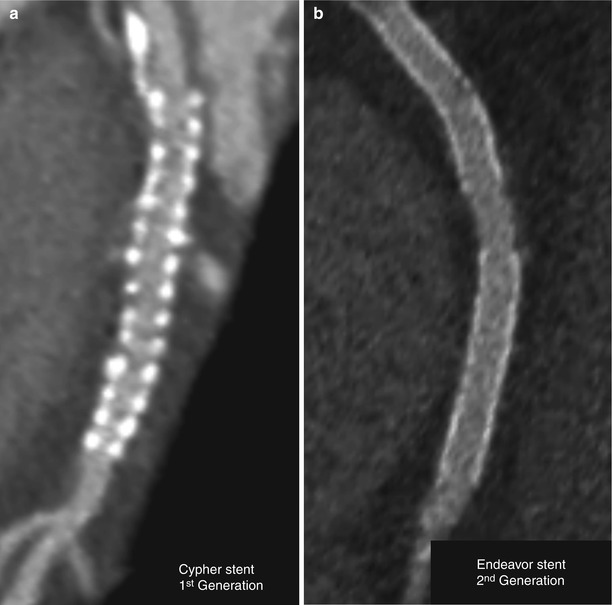
Fig. 8.1
First-generation (a) and second-generation DES on CT image. (a) Curved planar CT image of sirolimus-eluting stent (Cypher) shows relative thick strut. (b) Curved planar CT image of zotarolimus-eluting stent (Endeavor) shows thin strut
Table 8.3
First- and second-generation DES
Stent name
Drug
Metal
Polymer thickness (μm)
Strut thickness (μm)
Cypher
Sirolimus
Stainless steel
12.6
140
Taxus Express
Paclitaxel
Stainless steel
16.0
132
Taxus Liberte
Paclitaxel
Stainless steel
16.0
97
Endeavor
Zotarolimus
Cobalt chromium
4.1
91
Xience V
Everolimus
Cobalt chromium
7.6
81
8.2.2 Application of CTA for Coronary Stent Imaging
Reduction of motion artifact and achievement of optimal contrast enhancement of CT angiography are very important for stent imaging.
Image reconstruction and analysis tips for good quality of image.
Use sharp kernel reconstruction for reduction of blooming artifact (Fig. 8.2).
Use wide window of ≥700 HU with a center of about 200 HU for an acceptable trade-off between blooming and visibility of the stent lumen.
Use reconstruction mode of high spatial resolution, if available (Fig. 8.3).
Correct centerline of curved planar image carefully (Fig. 8.4).
Thick-slab maximal intensity projection (MIP) image may be helpful for delineation of a mechanical deformity (e.g., fracture) of the stent (Fig. 8.5).
Generate cross-sectional image of the stent to evaluate in-stent restenosis (Fig. 8.6).
Application of CTA for coronary stent [5]
In-stent restenosis
Mechanical deformity including stent fracture, longitudinal compression, and inadequate expansion
Edge stenosis and peri-stent plaque
Jailed branches
Late stent thrombosis
Bifurcation stents
Aneurysm of the coronary artery
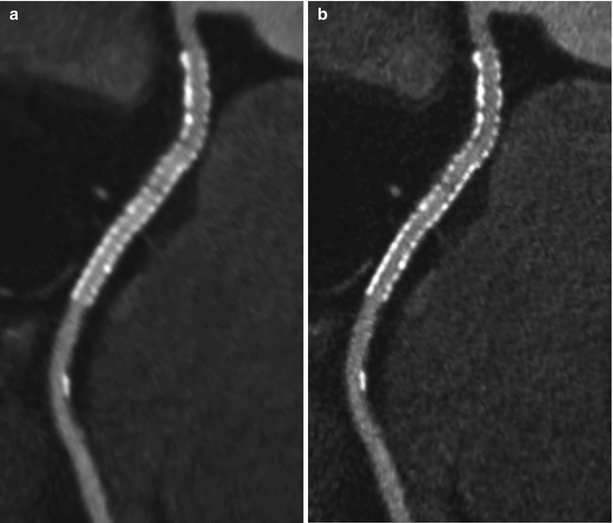
Fig. 8.2
Effect of image reconstruction kernel on image quality. Curved planar CT image of sirolimus-eluting stent (Cypher) with soft reconstruction kernel (B26; Siemens, Definition FLASH CT) (a) and sharp reconstruction kernel (B46) (b). In the sharp kernel image, blooming artifact from stent strut was markedly reduced as compared with that of soft kernel image
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


