The investigators report similar phenotypes of hypertrophic cardiomyopathy with left ventricular apical aneurysm and thrombus in 2 brothers aged 8 years apart. This report highlights the genetic predisposition for this unique, high-risk phenotype, the issue of prophylactic anticoagulation, and the importance of nonstandard echocardiographic imaging views in the assessment of these patients.
Case Description
Two brothers with hypertrophic cardiomyopathy (HC) were separately referred to our institution 2 weeks apart for evaluation. The older sibling, aged 68 years, had an implantable cardioverter-defibrillator placed 1 year before the visit, after an episode of sustained ventricular tachyarrhythmia. At his current visit, 2-dimensional transthoracic echocardiography showed a left ventricular (LV) apical aneurysm (3.1 × 1.2 cm) associated with an hourglass-shaped LV cavity formed because of midventricular hypertrophy, with no significant LV hypertrophy in the proximal or distal portions, and normal global systolic function ( Figure 1 , Video 1 ). Midsystolic muscular apposition of the hypertrophied septum and the lateral wall resulted in a midcavitary peak systolic gradient of 75 mm Hg. Standard imaging in the long-axis planes showed no evidence of thrombus. However, nonstandard oblique views in the 2-chamber long-axis orientation revealed a thrombus within the apical aneurysm ( Figure 1 , Video 2 ). The patient was in normal sinus rhythm at the time of the visit, with no history of atrial fibrillation.
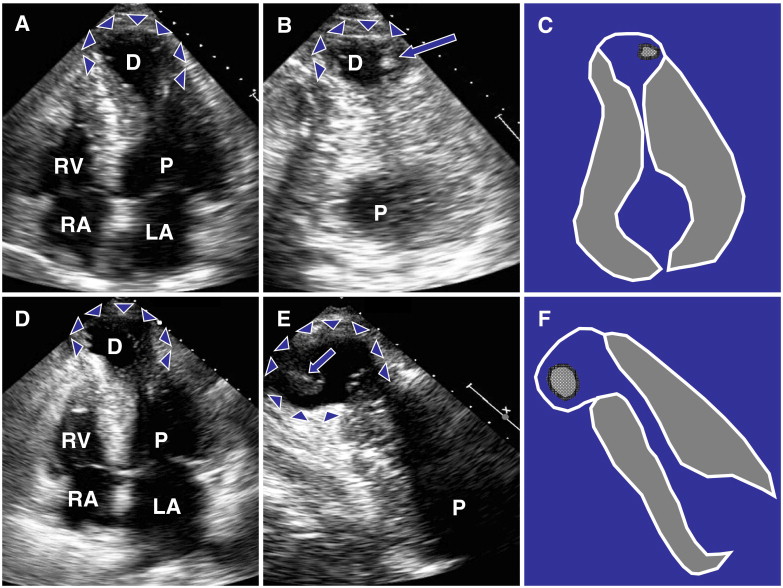
The previous patient’s younger brother, aged 60 years, also had an implantable cardioverter-defibrillator placed for primary prevention after an episode of syncope. Two-dimensional transthoracic echocardiography at his visit revealed an HC phenotype similar to that of his older brother, with a large LV apical aneurysm (4.6 × 2.8 cm) and an hourglass configuration of the LV cavity with hypertrophy localized to the midventricular septum and the lateral wall, producing a midcavitary peak systolic gradient of 20 mm Hg ( Figure 1 , Video 3 ) and moderately reduced LV systolic function (estimated ejection fraction 35%). As with his brother, although standard imaging in the long-axis planes did not demonstrate a thrombus in the apical aneurysm, nonstandard oblique views in the 2-chamber, long-axis orientation again revealed a large thrombus ( Figure 1 , Video 4 ). He also was in sinus rhythm during the visit and had no history of atrial fibrillation. The 2 brothers were initiated on warfarin therapy because of the risk for systemic thromboembolism.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


