Hypersensitivity, Eosinophilic, and Toxic Myocarditis
Hypersensitivity, Eosinophilic, and Toxic Myocarditis
Allen P. Burke, M.D.
Definitions
“Hypersensitivity myocarditis” is an etiologic definition that denotes a reaction to an ingested substance, usually a drug, that usually, but not always, has an eosinophilic reaction. “Eosinophilic myocarditis” is applied to symptomatic myocarditis with documented tissue or peripheral eosinophilia and often also has an allergic or hypersensitivity etiology. Eosinophils are not specific for cause, however, as they may be present in infectious as well as giant cell myocarditis.
Toxic myocarditis is a heterogeneous group of disorders. As is the case with hypersensitivity, drugs commonly cause toxic insults to the heart. However, the mechanism is believed to be direct myocyte toxicity, as opposed to immune-mediated mechanisms. Catecholamineinduced myocardial injury is often considered a form of toxic myocarditis, but because inflammation is relatively minimal, it is usually considered a form of cardiomyopathy (see Chapters 2 and 24). Chemotherapy-induced myocyte injury often goes through an inflammatory phase, but is also considered a form of cardiomyopathy (see Chapters 2 and 19). Other toxic compounds, such as arsenic, have historically been linked to a form of myocarditis. For all intents and purposes, the term “toxic myocarditis” is of limited use currently and will be addressed only briefly in this chapter.
Hypersensitivity and Eosinophilic Myocarditis
Incidence
Symptomatic hypersensitivity myocarditis, especially when documented histologically, is rare and generally the subject of case reports. The incidence of incidental hypersensitivity myocarditis diagnosed initially at autopsy is high, about 2% to 5%, depending on the population and history of medication use. In patients awaiting transplant, who are often on multiple medications, the incidence is 2% to 7%, as diagnosed histologically in the explanted heart or left ventricular apex removed at time of assist device insertion.1,2
Pathogenesis
Hypersensitivity is due to a delayed hypersensitivity reaction, and not a toxic effect of the offending drug. It has been postulated that modified collagen may be a trigger for eosinophilic reaction and degranulation.3
Many drugs have been histologically associated with hypersensitivity myocarditis.4 A smaller number have been implicated in symptomatic hypersensitivity myocarditis diagnosed histologically (generally by endomyocardial biopsy) (Table 164.1).
In incidentally found hypersensitivity myocarditis at autopsy and explants, a specific drug is rarely identified, because of multiple medication history.
Eosinophilic myocarditis may also be the result of mechanisms other than hypersensitivity. Churg-Strauss syndrome, parasitic infection, and chronic eosinophilic leukemia can result in eosinophilic infiltrates in the myocardium, often with myocyte necrosis. In some patients, an underlying cause or offending agent is never found.26
Clinical Findings
Clinical manifestations of hypersensitivity myocarditis fall into two groups of patients: those diagnosed during life, who have severe, often life-threatening symptoms (more often termed “eosinophilic myocarditis),” and those diagnosed at explant or autopsy, who often have no symptoms. The term “acute necrotizing eosinophilic myocarditis” has been used for the most severe form of hypersensitivity myocarditis that causes rapidly progressive congestive heart failure.27,28
TABLE 164.1 Drugs Associated with Hypersensitivity Myocarditis Diagnosed Pathologically
aDiagnosed made at autopsy. Others in table were diagnosed by biopsy.
Patients with symptomatic hypersensitivity myocarditis often present with signs and symptoms of myocarditis, often with heart failure. The symptoms generally occur within weeks after exposure to agent and generally resolve after withdrawal of the drug. The cardiac symptoms may be accompanied by a skin rash. Other manifestations of systemic hypersensitivity, including peripheral eosinophilia, may accompany hypersensitivity myocarditis (drug-induced rash with eosinophilia and systemic symptoms).5,21,29,30 Hypersensitivity myocarditis causing severe heart failure has been reported complicating Stevens-Johnson syndrome.19
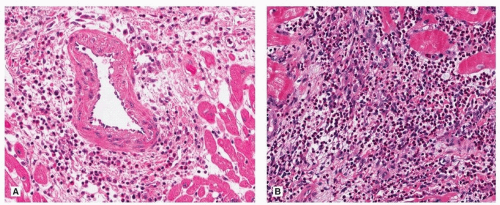
FIGURE 164.2 ▲ Hypersensitivity myocarditis. In this explanted heart in a transplant recipient, there are scattered interstitial infiltrates, without myocyte damage. A. There is interstitial inflammation with eosinophils and mononuclear cells. B. A higher magnification shows marked interstitial inflammation with prominent eosinophils.
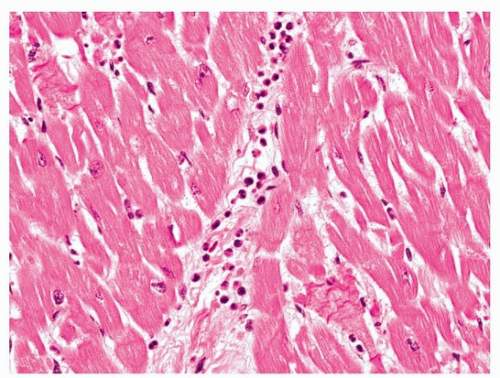
FIGURE 164.1 ▲ Hypersensitivity myocarditis. There is a sparse interstitial infiltrate, without any myocyte damage. Focal interstitial infiltrates are a common finding at autopsy, especially in patients on multiple medications.
Most patients respond to steroids and drug cessation.22,23,25,31,32 Irreversible heart failure may lead to cardiogenic shock and death, or heart transplantation.7,19,20
Only gold members can continue reading. Log In or Register to continue