Chapter 41
Hypercholesterolemia
1. Who should be screened for hypercholesterolemia?
2. True or false: Coronary atherosclerosis is common in persons in their 20s and 30s.
3. What are the ATP III classifications of LDL cholesterol, total cholesterol, HDL cholesterol, and triglyceride levels based on measured values?
The values, as denoted in ATP III, are given in Table 41-1. Note that since publication of this classification in 2001, a goal of LDL less than 70 mg/dL has emerged as desirable in some very high-risk populations and thus an LDL of significantly less than 100 mg/dL would now be considered optimal in such patients. To convert the values in the table to mmol/L, divide by 88.6.
TABLE 41-1
NCEP-ATP III CLASSIFICATION OF LDL, TOTAL CHOLESTEROL, HDL CHOLESTEROL, AND TRIGLYCERIDE LEVELS∗
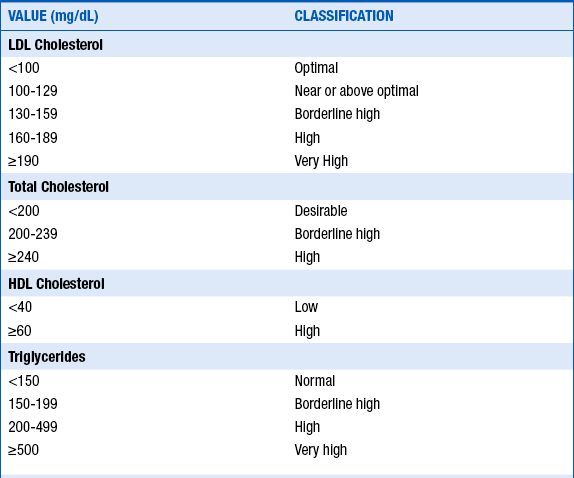
To convert mg/dL to mmol/L, divide by 88.6.
∗Note that since publication of this classification, a goal of LDL less than 70 mg/dL has emerged as desirable in some very-high risk populations.
Modified from Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults: Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 285:2486-2497, 2001.
4. What are important secondary causes of hypercholesterolemia?



 Chronic renal failure or nephrotic syndrome
Chronic renal failure or nephrotic syndrome
 Drugs (e.g., progestins, anabolic steroids, or corticosteroids)
Drugs (e.g., progestins, anabolic steroids, or corticosteroids)
A lipoprotein is the particle that transports cholesterol and triglycerides. Lipoproteins are composed of proteins (called apolipoproteins), phospholipids, triglycerides, and cholesterol (Fig. 41-1).
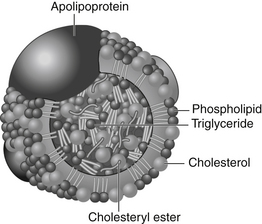
Figure 41-1 A lipoprotein particle. The polar surface coat is composed of apoproteins, phospholipids, and free cholesterol. The nonpolar lipid core is composed of cholesterol esters and triglycerides. (From Genest J, Libby P: Lipoprotein disorders and cardiovascular disease. In Libby P, Bonow RO, Mann DL, Zipes DP, editors: Braunwald’s heart disease: a textbook of cardiovascular medicine, ed 8, Philadelphia, 2008, Saunders.)
7. What is the minimal LDL goal for secondary prevention?
The minimal LDL goal for secondary prevention in patients with established coronary artery disease (CAD) is an LDL less than 100 mg/dL. This is also now the goal in patients with coronary heart disease risk equivalents (see Question 8). In an update to ATP III, it was emphasized that an LDL less than 100 mg/dL is a minimal goal of therapy. In light of more recent studies (Pravastatin or Atorvastatin Evaluation and Infection Therapy [PROVE-IT], Heart Protection Study [HPS], and Treating to New Targets [TNT]), a goal of LDL less than 70 mg/dL should be considered in patients with coronary heart disease at very high risk. Patients with coronary heart disease classified as very high risk include those with the following:
 Multiple major coronary risk factors (especially diabetes)
Multiple major coronary risk factors (especially diabetes)
 Severe and poorly controlled risk factors (especially continued cigarette smoking)
Severe and poorly controlled risk factors (especially continued cigarette smoking)
 Multiple risk factors of metabolic syndrome (see Question 9)
Multiple risk factors of metabolic syndrome (see Question 9)

8. What is a coronary heart disease risk equivalent?





