Fig. 11.1
Hybrid operating room: this is a modern hybrid operating room with advanced robotic arm imaging capabilities—(Bon Secours St. Mary’s Hospital, Richmond, Virginia) (Photo by Doug Buerlein Photography; used with permission)
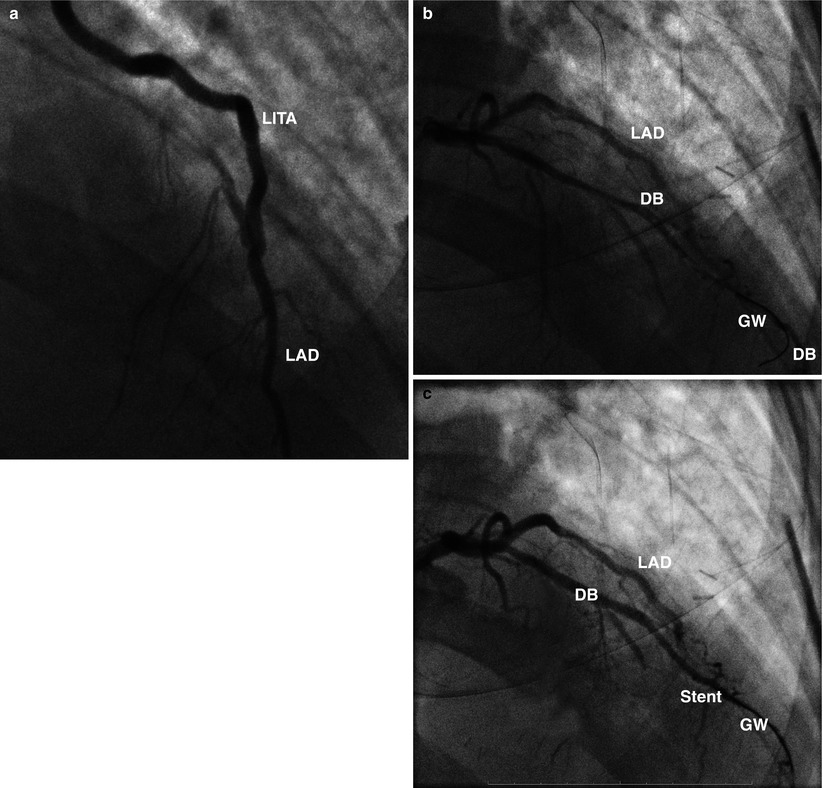
Fig. 11.2
Hybrid TECAB—PCI: (a) This completion angiogram was performed in the hybrid operating room immediately after the left anterior descending coronary (LAD) artery was grafted with a left internal thoracic artery (LITA), using robotic techniques. In this patient the LAD surgical grafting was followed the next day with PCI therapy to other vessels. (b) Interval PCI of a diagonal branch (DB): Guide-wire (GW) for stent placement in a diagonal branch (DB). Competitive blood flow from an earlier robotic left internal thoracic artery to LAD graft is shown in left anterior descending coronary artery. (c) In this hybrid revascularization case a stent has been placed in the distal diagonal branch (DB). GW guide-wire, LAD left anterior descending coronary artery
Logistic issues that are related to procedural timing and/or the interventional sequence are dependent upon several factors. If a PCI is performed first, the anterior ventricular territory is protected for the subsequent procedure. However, the ensuing surgical revascularization often must be delayed weeks to months because of platelet activity inhibition, which is needed to preserve patency of coronary stents. This is especially true if drug-eluting stents have been deployed earlier, as they require a longer period of continuous antiplatelet therapy. It should be recognized that anticoagulation reversal, following a robotic surgical procedure, increases the risk of thrombosis of both fresh and interval stents.
Conversely, if the AH-TECAB is the initial procedure, anti-platelet therapy is begun post-operatively and remains helpful during the interval PCI. Moreover, when a coronary stent has been deployed, following anterior ventricular wall grafting, completion ITA to LAD angiography can be performed to confirm graft patency and sufficient distal coronary blood flow. Nevertheless, if PCI complications occur with this revascularization sequence, surgical intervention becomes more difficult because of the incumbent re-operative setting.
AH-TECAB: Operative Planning and Set-Up
Robotic hybrid procedures can be performed using several different coronary-grafting strategies. These include a robotic ITA harvest followed by (1) a “hand-sewn” minimally invasive direct coronary artery bypass (MIDCAB) anastomosis, (2) an arrested heart TECAB, or (3) a beating heart (BH) TECAB (with or without perfusion assistance). For most patients the author prefers to perform a subsequent AH-TECAB. (See Chap. 7). Generally, the AH-TECAB method provides, short perfusion and aortic cross clamp times, as well as excellent visibility with an adequate intra-thoracic workspace. It is the ideal technique to provide an unencumbered and accurate anastomosis. Nevertheless, the other methods just described remain in our armamentarium for specific situations. (See Chap. 8).
For an AH-TECAB the patient is positioned toward operating table left side with the left arm supported by a draw sheet. A roll is placed beneath the left chest and inferior to the scapular tip. This position helps spread the intercostal spaces as the left shoulder drops posteriorly. Thereafter, the table is tilted 30° to the patient’s right side. The robotic instrument cart is placed on the right side of the operating table. When positioning instrument tables and perfusion equipment, sufficient space must be reserved for the robotic instrument cart.
AH-TECAB: Anesthetic Considerations
Standard cardiac anesthetic protocols are used and include single lung ventilation with either a double-lumen endotracheal tube or a bronchial blocker. In some cases a pulmonary artery vent is placed percutaneously via the right internal jugular vein to maintain a dry operative field. When using Endo-aortic™ balloon occlusion, bilateral radial arterial lines are essential to avoid the possibility of distal balloon migration, possibly covering the innominate artery origin. Routine trans-esophageal echocardiography is used to monitor Endo-aortic™ balloon placement and continued position as well as postoperative cardiac function. Defibrillator pads are placed anterior to right shoulder and along the left costal margin posteriorly.
AH-TECAB: Instrument Port Placement
The camera port is placed in the left 5th intercostal space between the nipple and anterior axillary line. Carbon dioxide insufflation is begun to facilitate adequate intra-thoracic operative visualization. Early identification of the LITA and vein, left subclavian vessels, and the phrenic nerve is very important. Insuflation CO2 pressures should be kept between 8 and 12 cm H2O to maintain an adequate, safe anterior pericardial working space. Careful observation for hemodynamic alterations is necessary when increasing the CO2 intra-thoracic pressure.
The right and left instrument arm ports are placed in the left 3rd and 7th intercostal spaces, respectively, either in line with the camera port or just lateral to it. A good guide for right instrument arm placement is midway between the male left nipple and tip (acromion) of the left shoulder. The left shoulder is the most common anatomic point for external robotic arm conflict in these cases. For beating heart or off pump TECAB surgery, a 4th arm port is inserted to the left of the xiphoid process and along the costal margin for introduction of the 10-mm endo-stabilizer. All ports and instruments should be introduced under clear endoscopic visualization. Creation of an additional port is optional for passing supplies and external assistance. We pass supplies routinely into the thoracic cavity via the right arm port. A 12-mm port, instead of the standard 8-mm one, allows the flow probe cable to pass beside the right instrument arm the end of the procedure. After port placement the daVinci™ instrument cart is deployed tableside for instrument docking. For an AH-TECAB the center of the cart should be aligned with the camera port. When using an endo-stabilizer, instrument cart centerline alignment with either the right instrument port or left shoulder may help avoid external conflicts.
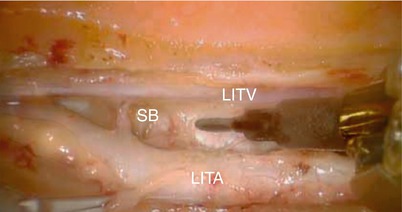
AH-TECAB: ITA Takedown and Preparation
For this part of the operation, we prefer to use either the micro or bipolar robotic forceps and the spatula cautery. Endoscopic magnification allows a very precise dissection that facilitates the ITA harvest greatly with or without skeletonization (Fig. 11.3). The latter method avoids the need either for coagulation or clipping venous branches and can result in a significantly longer graft. The electrocautery should be set on low power (i.e., 15 W) to avoid undesired thermal tissue conduction. Even in obese patients, a portion of the ITA usually is visible along the chest wall. The dissection is started in this area by incising the endothoracic fascia, just lateral to the artery, which allows the dissected tissue to fall away from the endoscope. Most branches can be cauterized and then divided, leaving robotic instrument clip application either for large and/or more difficult tributaries. The dissection is carried cephalad to where the phrenic nerve crosses the ITA and caudally to the intramuscular arterial bifurcation. The ITA is left intact while the pericardial fat is reflected laterally to expose the pericardium, which then is opened to identify the LAD. To ensure correct LAD identification, care should be taken to identify the left atrial appendage and appropriate diagonal branches.