Chapter 23
Heart Failure Evaluation and Long-Term Management
Arunima Misra, MD, FACC, Kumudha Ramasubbu, MD, FACC, Shawn T. Ragbir, MD, Glenn N. Levine, MD, FACC, FAHA and Biykem Bozkurt, MD, PhD, FACC, FAHA
This chapter deals specifically with the evaluation and long-term management of patients with heart failure caused by depressed ejection fraction. The management of patients with heart failure with preserved ejection fraction (diastolic dysfunction) is discussed in Chapter 24. The management of patients with acute decompensated heart failure is discussed in Chapter 22. Specific discussions of the evaluation and management of myocarditis, dilated cardiomyopathy, hypertrophic cardiomyopathy, and restrictive/infiltrative cardiomyopathy, as well as consideration with cardiac transplantation, are discussed in other dedicated chapters in this section of the book. The roles of pacemakers and implantable cardioverter-defibrillators in patients with heart failure are discussed in this chapter, as well as in the chapters on pacemakers (Chapter 37) and implantable cardioverter-defibrillators (Chapter 38).
1. What are the most common causes of heart failure?
2. What elements should the initial assessment of the patient with heart failure include?
Initial assessment of the patient with heart failure should include:
 Evaluation of heart failure symptoms and functional capacity (dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea [PND], fatigue, and lower extremity edema)
Evaluation of heart failure symptoms and functional capacity (dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea [PND], fatigue, and lower extremity edema)


 Laboratory tests, including complete blood cell count (CBC), creatinine and blood urea nitrogen (BUN), serum electrolytes, natriuretic peptide (BNP or NT-proBNP), fasting blood glucose, lipid profile, liver function tests, thyroid-stimulating hormone (TSH), and urine analysis; and screening for hemochromatosis and human immunodeficiency virus (HIV), pheochromocytoma, amyloidosis, or rheumatologic diseases reasonable in selected patients, particularly if there is clinical suspicion for testing
Laboratory tests, including complete blood cell count (CBC), creatinine and blood urea nitrogen (BUN), serum electrolytes, natriuretic peptide (BNP or NT-proBNP), fasting blood glucose, lipid profile, liver function tests, thyroid-stimulating hormone (TSH), and urine analysis; and screening for hemochromatosis and human immunodeficiency virus (HIV), pheochromocytoma, amyloidosis, or rheumatologic diseases reasonable in selected patients, particularly if there is clinical suspicion for testing






3. How are heart failure symptoms classified?
 Class I: No limitation; ordinary physical activity does not cause excess fatigue, shortness of breath, or palpitations.
Class I: No limitation; ordinary physical activity does not cause excess fatigue, shortness of breath, or palpitations.

 Class III: Marked limitation of physical activity; ordinary activity will lead to symptoms.
Class III: Marked limitation of physical activity; ordinary activity will lead to symptoms.

4. What is the stage system for classifying heart failure?
In 2001, the American College of Cardiology/American Heart Association (ACC/AHA) introduced a system to categorize the stages of heart failure. This system is somewhat different in focus than the previous NYHA classification system and was intended, in part, to emphasize the prevention of the development of symptomatic heart failure. In addition, the 2009 update on the 2005 Heart Failure Guidelines suggest appropriate therapy for each stage (Figure 23-1).
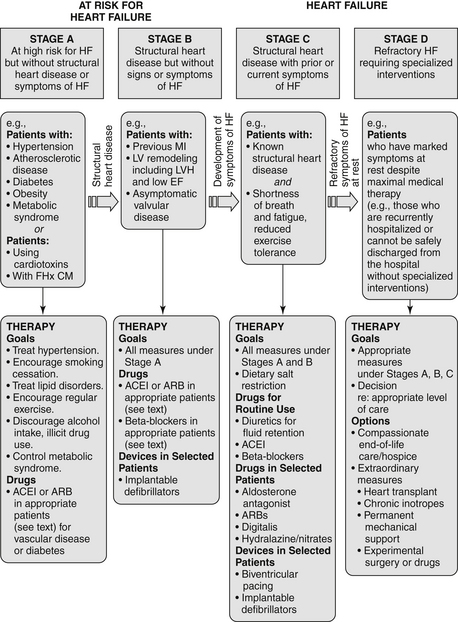
Figure 23-1 American College of Cardiology/American Heart Association Stages in the Development of Heart Failure/Recommended Therapy by Stage. (From Jessup M, Abraham WT, Casey DE, et al: ACC/AHA 2009 focused update: ACCF/AHA guidelines for the diagnosis and management of heart failure in adults : a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: Developed in collaboration with the International Society for Heart and Lung Transplantation, Circulation 119:1977-2016, 2009; originally published online March 26, 2009.) ACEI, Angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; EF, ejection fraction; FHx CM, family history of cardiomyopathy; HF, heart failure; LV, left ventricle; LVH, left ventricular hypertrophy; MI, myocardial infarction.
 Stage A: Patient is at high risk for developing heart failure but is without structural heart disease or symptoms of heart failure. Includes patients with hypertension, coronary artery disease (CAD), obesity, diabetes, history of drug or alcohol abuse, history of rheumatic fever, family history of cardiomyopathy, or treatment with cardiotoxins
Stage A: Patient is at high risk for developing heart failure but is without structural heart disease or symptoms of heart failure. Includes patients with hypertension, coronary artery disease (CAD), obesity, diabetes, history of drug or alcohol abuse, history of rheumatic fever, family history of cardiomyopathy, or treatment with cardiotoxins

 Stage C: Patient with structural heart disease and with prior or current symptoms of heart failure
Stage C: Patient with structural heart disease and with prior or current symptoms of heart failure
 Stage D: Patient with refractory heart failure requiring specialized interventions
Stage D: Patient with refractory heart failure requiring specialized interventions
5. Which patients with heart failure should be considered for endomyocardial biopsy (EMB)?
In 2007, the ACC/AHA/European College of Cardiology (ACC/AHA/ECC) issued a scientific statement on the role of EMB. Most patients who are seen for heart failure should not be referred for EMB. Biopsy results are often nonspecific or unrevealing, and in most cases there is no specific therapy based on biopsy results that have been shown to improve prognosis. However, in certain clinical scenarios, EMB should be performed (class I recommendation) or can be considered and is considered reasonable (class IIa recommendation). As given in that document, these scenarios include the following:
 New-onset heart failure of less than 2 weeks duration associated with a normal-sized or dilated left ventricle and hemodynamic compromise (class I; level of evidence B)
New-onset heart failure of less than 2 weeks duration associated with a normal-sized or dilated left ventricle and hemodynamic compromise (class I; level of evidence B)



 Heart failure associated with suspected anthracycline cardiomyopathy (class Ia; level of evidence C)
Heart failure associated with suspected anthracycline cardiomyopathy (class Ia; level of evidence C)
 Heart failure with unexplained restrictive cardiomyopathy (class IIa; level of evidence C)
Heart failure with unexplained restrictive cardiomyopathy (class IIa; level of evidence C)
6. What are the general treatments for patients with heart failure?
 Diuretics are indicated for volume overload. Starting doses of furosemide are often 20 to 40 mg once or twice a day, but higher doses will be required in patients with significant renal dysfunction. The dose should be uptitrated to a maximum of up to 600 mg daily in divided doses. Failure of therapy is often the result of inadequate diuretic dosing. Torsemide is more expensive than furosemide but has superior absorption and longer duration of action. Bumetanide is approximately 40 times more potent milligram-for-milligram than furosemide and can also be used in patients who are unresponsive or poorly responsive to furosemide. Synergistic diuretics that act on the distal portion of the tubule (thiazides such as metolazone, or potassium-sparing agents) are often added in those who fail to respond to high-dose loop diuretics alone. In addition, a new recommendation from 2009 Focused Update states that for hospitalized heart failure patients, if diuresis is inadequate to relieve congestion, higher doses of loop diuretics should be used, addition of second diuretic should be made or continuous infusion of a loop diuretic should be considered.
Diuretics are indicated for volume overload. Starting doses of furosemide are often 20 to 40 mg once or twice a day, but higher doses will be required in patients with significant renal dysfunction. The dose should be uptitrated to a maximum of up to 600 mg daily in divided doses. Failure of therapy is often the result of inadequate diuretic dosing. Torsemide is more expensive than furosemide but has superior absorption and longer duration of action. Bumetanide is approximately 40 times more potent milligram-for-milligram than furosemide and can also be used in patients who are unresponsive or poorly responsive to furosemide. Synergistic diuretics that act on the distal portion of the tubule (thiazides such as metolazone, or potassium-sparing agents) are often added in those who fail to respond to high-dose loop diuretics alone. In addition, a new recommendation from 2009 Focused Update states that for hospitalized heart failure patients, if diuresis is inadequate to relieve congestion, higher doses of loop diuretics should be used, addition of second diuretic should be made or continuous infusion of a loop diuretic should be considered.





The elements of long-term management of patients with CHF resulting from depressed LV systolic function are summarized in Table 23-1.
TABLE 23-1
ELEMENTS OF THE LONG-TERM MANAGEMENT OF PATIENTS WITH CONGESTIVE HEART FAILURE DUE TO LEFT VENTRICULAR SYSTOLIC DYSFUNCTION
| Treatment/Intervention | Recommendation (Level of Evidence) |
| Diuretics for fluid retention | Class I (LOE: C) |
| Salt restriction | Class I (LOE: C) |
| ACE inhibitors (ACEIs) | Class I (LOE: A) |
| Angiotensin II receptor blockers (ARB) in ACEI-intolerant patients | Class I (LOE: A) |
| ARB in persistently symptomatic patients with reduced LVEF already being treated with conventional therapy | Class IIb (LOE: C) |
| Hydralazine + Isosorbide in patients ACEI and ARB intolerant | Class IIb (LOE: C) |
| Hydralazine + Isosorbide in patients already on ACEI and β-blocker with persistent symptoms | Class IIa (LOE: A) |



