Chapter 3 Heart failure and cardiomyopathy
Introduction
Heart failure is a complex syndrome in which the heart functions inadequately as a pump to support a physiological circulation resulting in symptoms such as breathlessness and fatigue and signs such as fluid retention. It is associated with high morbidity and mortality and represents a major burden for healthcare services.
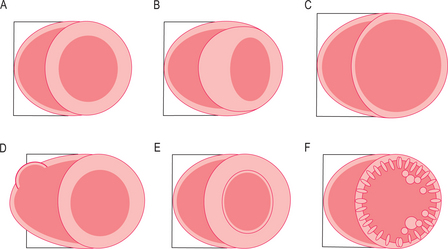
The cardiomyopathies are diseases of the myocardium associated with cardiac dysfunction and are subdivided on the basis of morphology into hypertrophic, dilated, restrictive and ARVC (Figure 3.1). Many cardiomyopathies are inherited through a single gene abnormality. Some cardiomyopathies have an extended phenotype with conduction disease, whilst other genetic cardiac diseases have conduction disease (such as long/short QT and the Brugada syndrome—the channelopathies) without ‘cardiomyopathy’. At least nine different sarcomeric genes can cause the same phenotype of hypertrophic cardiomyopathy (HCM) and yet different mutations in some of these nine genes can also cause DCM. Approximately half of all HCM patients have been shown to have a genetic mutation and many individuals carry mutations without phenotypic manifestation, and the impact of environment, genetic modifiers and patient age are important. There are also disease mimics known as phenocopies, such as the glycogen storage diseases, which appear phenotypically like the genetic diseases.
CMR protocol
A CMR heart failure and cardiomyopathy protocol typically obtains information on cardiac morphology, cardiac function and myocardial tissue characterization. The scan report should comment on these three areas in general terms such as:
Specific features for reporting are highlighted after discussion of the specific cardiomyopathies.
Cardiac function
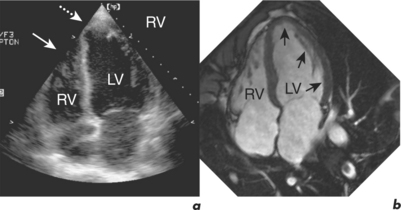
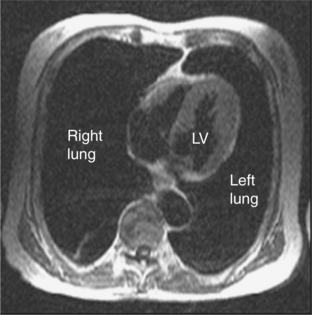
CMR is the gold standard technique for the assessment of left and right ventricular volumes and mass due to a combination of advantages (Table 3.1). CMR measurements are more reproducible than echocardiography, the apex and RV are no longer blind spots (Figure 3.2), and the technique is not window dependent (Figure 3.3). For heart failure, the SSFP GE cine sequences have major advantages because the blood to myocardium contrast is dependent not on blood flow but on intrinsic magnetic differences between blood and myocardium. This means that the blood pool is more clearly distinguished from myocardium even in slow-flow areas compared to that using older white-blood imaging methods. The SSFP sequences can also be sped up using parallel imaging acquisition techniques to minimize breath-holding times in symptomatic heart failure patients.
Table 3.1 Advantages of CMR for measuring ventricular function
| Precise and reproducible piloting |
| No problems with acoustic windows |
| No blind spots—image quality the same throughout |
| High blood–myocardial tissue contrast (even in heart failure) |
| True 3D assessment with no geometric assumptions |
| RV imaged as well as the LV |
| Any view or plane can be imaged as necessary |
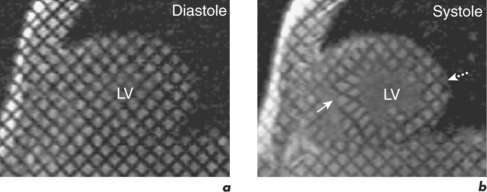
An emerging technique for functional assessment is myocardial tagging. In this technique, a grid of tag lines is laid over the heart magnetically in diastole and then tracked as they distort with myocardial contraction through systole (Figure 3.4). The tag line deformation can be analysed like tissue Doppler imaging, but rather than being limited to strain in line with the Doppler beam, tagging can be analysed in any direction simultaneously, including circumferentially, at any point in the myocardium, and is able to compare epicardial and endocardial function.
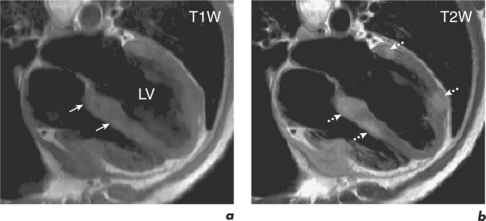
Myocardial tissue characterization
Normal and abnormal myocardium can have intrinsic contrast differences in heart failure that can be visualized by CMR. For example, fatty infiltration of the RV may be seen in ARVC using FSE sequences with and without the addition of a specially applied fat saturation pulse, which eliminates only fat from the images. Also, tissues which have increased water content, such as in myocardial oedema from acute infiltration or infarction, can be differentiated with T2W sequences (Figure 3.5). Extrinsic contrast can be created by LGE, which uses an inversion recovery sequence and a gadolinium contrast agent (see Chapter 2). Gadolinium highlights areas of myocardium with expanded interstitium, such as fibrosis, necrosis or infiltration. Different patterns of fibrosis exist in different aetiologies of heart failure and this can be used to distinguish them (Figure 3.6). MI leads to patterns of LGE which spread from the subendocardium outward to the subepicardium in the territory of a coronary artery. However, changes in myocarditis are the reverse and start at the subepicardium and can later become mid-myocardial, typically at the lateral wall. EGE in combination with relevant cines allows identification of thrombi. This technique has been discussed in the previous chapter and will also be covered in Chapter 5 on cardiac masses. Coronary CMR assessment of the proximal coronary arterial tree can be combined with myocardial tissue characterization but this technique is not robust—it is further discussed in Chapter 9.