Chapter 51
Heart Disease in Pregnancy
1. What cardiac physiologic changes occur during pregnancy?
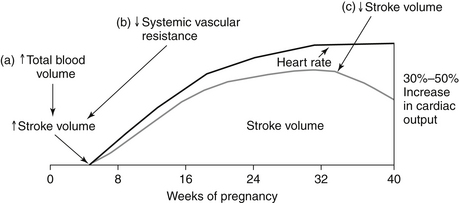
Hormonal changes cause an increase in both plasma volume (from water and sodium retention) and red blood cell volume (from erythrocytosis) during a normal pregnancy. A disproportionate increase in plasma volume explains the physiologic anemia of pregnancy. Maternal heart rate (HR) increases throughout the 40 weeks, mediated partially by increased sympathetic tone and heat production. Stroke volume subsequently continues to increase until the third trimester, when inferior vena cava (IVC) return may be compromised by the gravid uterus. Maternal cardiac output increases by 30% to 50% during a normal pregnancy. Systolic blood pressure drops during the first half of pregnancy and returns to normal levels by delivery. The physiologic changes related to cardiac output that occur during pregnancy are shown in Figure 51-1.
2. Are there independent vascular changes that occur during a normal pregnancy?
3. What are normal cardiac signs and symptoms of pregnancy?
 Hyperventilation (as a result of increased minute ventilation)
Hyperventilation (as a result of increased minute ventilation)
 Peripheral edema (from volume retention and vena caval compression by the gravid uterus)
Peripheral edema (from volume retention and vena caval compression by the gravid uterus)
 Dizziness/lightheadedness (from reduced SVR and vena caval compression)
Dizziness/lightheadedness (from reduced SVR and vena caval compression)

4. What are pathologic cardiac signs and symptoms of pregnancy?
 Anasarca (generalized edema) and paroxysmal nocturnal dyspnea are not components of normal pregnancy and warrant workup.
Anasarca (generalized edema) and paroxysmal nocturnal dyspnea are not components of normal pregnancy and warrant workup.



5. What are normal cardiac examination findings during pregnancy?
 Blood pressure (BP) will decline and HR will increase.
Blood pressure (BP) will decline and HR will increase.
 The point of maximum impulse will be displaced laterally as the uterus enlarges.
The point of maximum impulse will be displaced laterally as the uterus enlarges.

 A physiologic pulmonic flow murmur is common because of elevated stroke volume passing through a normal valve.
A physiologic pulmonic flow murmur is common because of elevated stroke volume passing through a normal valve.

6. What are pathologic cardiac exam findings during pregnancy?
 Clubbing and cyanosis are not a part of normal pregnancy; desaturation for any reason is abnormal and warrants investigation.
Clubbing and cyanosis are not a part of normal pregnancy; desaturation for any reason is abnormal and warrants investigation.



 Audible S4 is unusual during pregnancy and may reflect underlying hypertension.
Audible S4 is unusual during pregnancy and may reflect underlying hypertension.
7. What are the cardiac changes that occur during labor and delivery?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


