Fig. 15.1
A large P2 posterior leaflet with nearly all edge chords ruptured (flail leaflet). Here, P2 functions independent (clefts) of adjacent P1 or P3 scallops. There is no support from lateral leaflet scallop chords. The cartoon suggests that an elongated P2 with many ruptured chords needs a “haircut”
The redundant P2 segment is identified best by ventricular saline pressure filling (saline test). Then it is extended to the full length and the redundant portion removed (Fig. 15.2). The height (length from annulus) of P1 and P2 are used to gauge the ultimate length of the P2 remainder. The end of P2 is resected by amputating the end of the scallop to the length of P1 and P3. Any stable good quality chords attached to P2 are identified and preserved along with a small leaflet segment.
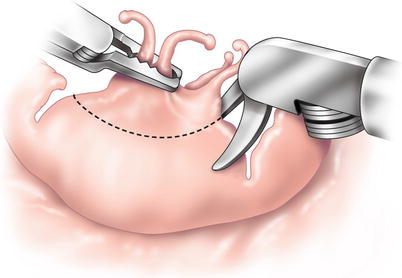
Fig. 15.2
Robotic scissors trim the leading edge of P2 (with ruptured chords) to a length equaling that of P1 and P3, achieving a uniform posterior leaflet height. Elongated but intact chords may remain on each side of a flail P2. Medial transfer of these toward the center will reduce leaflet prolapse. Any good P2 chords are preserved with an island of leaflet tissue
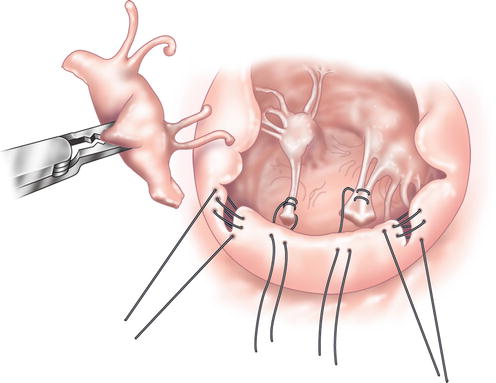
In Fig. 15.3, intact chords are re-approximated to the “new” coapting edge of P2. By rotating lateral chords toward the center of P2, any residual prolapse becomes reduced toward the ventricle. At this time “clefts” between P1 and P2 or P2 and P3 are closed, adding additional chordal support to P2. Finally, an appropriately sized annuloplasty band or ring is implanted using interrupted 2-0 braided mattress sutures (Fig. 15.4). This shortens the posterior annulus and creates greater leaflet coaptation.