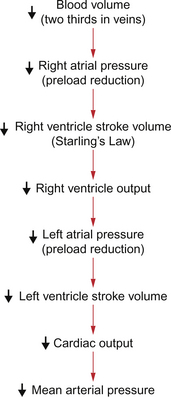
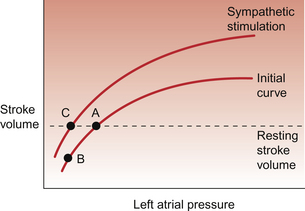
14 Blood volume in the textbook subject is of the order of 5 L (see Chapter 1) and at any one time about 65% of this volume is in the venous compartment of the circulation. A reduction in blood volume may occur in many ways. Loss of whole blood through blood vessel trauma either directly out of the subject or into other tissues such as the lumen of the stomach or a thigh muscle is referred to as haemorrhage. However, excessive vasodilatation of peripheral blood vessels will induce similar physiological responses to loss of blood volume. These processes increase the ‘volume’ of the circulatory system whilst the volume of blood it contains remains unchanged leading to a relative hypovolaemia. Normal physiological compensatory responses will usually cope with low levels of blood loss (up to 10% blood volume) without problem. This happens frequently on a voluntary basis with people who lose 500 mL blood while attending a blood donor session. The fundamentals of these physiological responses are firstly short-term maintenance of arterial blood pressure so that tissue perfusion is sustained and, secondly, over a longer time course, the lost blood volume is replaced. These mechanisms, which link together many of the individual topics covered in greater detail earlier in this book, will now be reviewed. Severe insults to the circulatory system lead to the syndrome of circulatory shock. This topic is discussed at the end of this chapter. A case history of a patient who has suffered a haemorrhage is shown in Case 14.1:1. Rapid (time course in minutes) blood volume losses of the order of 5–10% in someone with normally functioning circulatory reflexes produce little if any change in mean arterial pressure. A rapid 15–20% haemorrhage will cause a modest reduction in mean arterial pressure from a normal textbook value of about 93 mm Hg (see Chapter 9) to about 80–90 mm Hg. Recovery from such a haemorrhage using normal physiological mechanisms should be uneventful. A 20–30% blood volume loss might typically result in a drop in mean arterial blood pressure to 60–80 mm Hg and generate some indications of shock responses but such a haemorrhage would not normally be fatal. A blood volume loss of 30–40% however would lead to a substantial reduction of mean arterial blood pressure to 50–70 mm Hg with serious shock responses which may become irreversible. Blood volume loss beyond 50% would normally be fatal. The fundamental links between blood loss and hypotension are described in Chapter 4 and are summarized in Figure 14.1. Decreased blood volume leads to decreased right atrial pressure and consequently decreased filling of the right ventricle. This leads to a decrease in stroke volume (Starling’s law) and therefore to a reduction in cardiac output. A 20% reduction in blood volume would typically result in an initial reduction in resting cardiac output from about 5 L/min to about 3 L/min. As mean arterial pressure is the product of cardiac output and peripheral resistance there is a fall in blood pressure as identified above. An important first aid point is that it is inadvisable to prop up someone who has suffered a haemorrhage to a sitting position. This would only further reduce the preload effects on the heart. The compensatory responses which would help to restore blood pressure are triggered by the cardiovascular reflexes discussed in Chapter 10. Of prime importance is the carotid sinus baroreceptor reflex. The modified nerve endings which constitute the baroreceptor become less stretched as blood pressure falls. Fewer action potentials will therefore pass up the glossopharyngeal nerve and enter the brain at the level of the medulla. Following central processing of the baroreceptor input there will be activation of sympathetic outflow and inhibition of the parasympathetic nerve supply to the heart. The consequences are an increased heart rate (tachycardia) and an increase in cardiac contractility, both of which contribute to a raised cardiac output despite decreased preload effects on the heart (see Chapter 4). Re-establishment of a normal resting stroke volume as a result of a sympathetically induced increase in cardiac contractility is illustrated in Figure 14.2. In otherwise normal subjects, a significant tachycardia does not occur until the blood loss has exceeded 700–800 mL (10–15%). Sympathetic nervous system activation also leads toα-receptor-mediated vasoconstriction (see Chapter 9). The regions of the circulation which are particularly affected by sympathetic vasoconstriction responses include the skin, gut, kidney and skeletal muscle. The brain and coronary circulations are relatively preserved especially during the sequel to a haemorrhage amounting to about 20% or less blood volume loss. Concurrent sympathetically mediated venoconstriction will help to maintain central venous pressure and hence limit the fall in preload on the right side of the heart. An unfortunate practical aspect of this venoconstriction is that it may hinder attempts to gain access to the circulation with a venous cannula so that infusion of blood or other replacement body fluids can commence. The patient who has suffered a haemorrhage and has therefore activated these compensatory responses appears pallid due to cutaneous vasoconstriction, with cold clammy skin, possibly with peripheral cyanosis, and a weak rapid pulse. The responses to haemorrhage will vary considerably between individuals depending on factors such as age and gender, nutrition and fluid balance, season of the year and environmental temperature as well as less easily defined individual characteristics. The extent and speed of the haemorrhage will be important as well. When haemorrhage reaches levels of the order of 25–35% blood loss the sympathetic activation outlined above is succeeded by inhibition of sympathetic outflow and progression to circulatory shock as described later in this chapter. Peripheral cyanosis (see Chapter 1) is associated with a reduced local blood flow and hence greater than normal extraction of oxygen from the remaining blood. Sweating is regulated by the sympathetic nervous system and so is another manifestation of the baroreceptor reflex. Some of these autonomic nervous system mediated changes feature in the case history of Linda Hamilton outlined in Case 14.1:1. A simple but quite effective test of peripheral circulatory function is the nail capillary refill test. Pressure is applied to a finger nail bed until it has blanched. This indicates that blood has been forced away from the area. When pressure is removed the time taken for blood to return to the nail bed (indicated by a change in colour) is measured. Normally capillary refill time will be less than 2 seconds. A longer time indicates reduced tissue perfusion. This test is particularly useful in children as other signs of imminent circulatory collapse appear relatively late. In Chapter 11 the ‘Starling forces’ which determine the movement of water across capillary walls are described. Fundamentally, the capillary blood pressure (hydrostatic pressure) tends to move water out of the capillary bed into the interstitial fluid. This is opposed by a gradient of colloid osmotic pressure which will tend to draw water from the interstitial compartment back into the capillary. Following a haemorrhage, there may be a fall in mean arterial pressure but, in addition, a compensatory peripheral vasoconstrictor response occurs. As the main resistance vessels (see Chapter 9) are the arterioles, vessels which come immediately before the capillaries, there will be a fall in capillary blood pressure following a haemorrhage. This will alter the balance of the Starling forces and, as the colloid osmotic pressure of plasma is initially unchanged, this will result in a net movement of water from the interstitial space into the blood. This is illustrated in Figure 14.3. The rate and extent of this internal replacement of lost blood volume will depend on the rate and degree of blood loss. A rapid loss of 20% of blood volume (about a 1000 mL haemorrhage in the ‘textbook person’) will lead to perhaps 600 mL of interstitial fluid entering the blood over a period of around 10 minutes. This is sometimes referred to as an ‘internal transfusion’. As skeletal muscle constitutes about 50% of body weight this tissue is a major source of the interstitial fluid for the internal transfusion.
HAEMORRHAGE AND CIRCULATORY SHOCK
Introduction
Arterial blood pressure changes in response to haemorrhage
Short-term responses which help to restore lost blood volume
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine