Haemodialysis Access Haemodialysis patients need vessels that can be regularly cannulated and have large volumes of blood drained out of them (without collapsing) and large volumes of blood replaced back into them (without bursting). Unfortunately only central veins exist naturally that can perform these functions and perhaps the simplest way to haemodialyse a patient would be through a central line, which can be tunnelled under the skin (to reduce infection risk) into the internal jugular vein with its tip in the SVC. However, these occlude over time, they can become infected and they are thrombogenic, which can result in central vein occlusion. They are good as a short-term solution only. That’s where the surgically created AVF comes in. By joining an artery to a superficial vein, high-pressure blood is redirected up the vein back to the heart. Over time, this expands the vein, which becomes thick walled (‘arterialises’) and eventually, on average, a litre of blood may pass though the fistula every minute (this is very variable on the fistula and the patient but you would aim for >600 ml/min). Because patients may be on haemodialysis for many years, they may need several over time because they may thrombose.
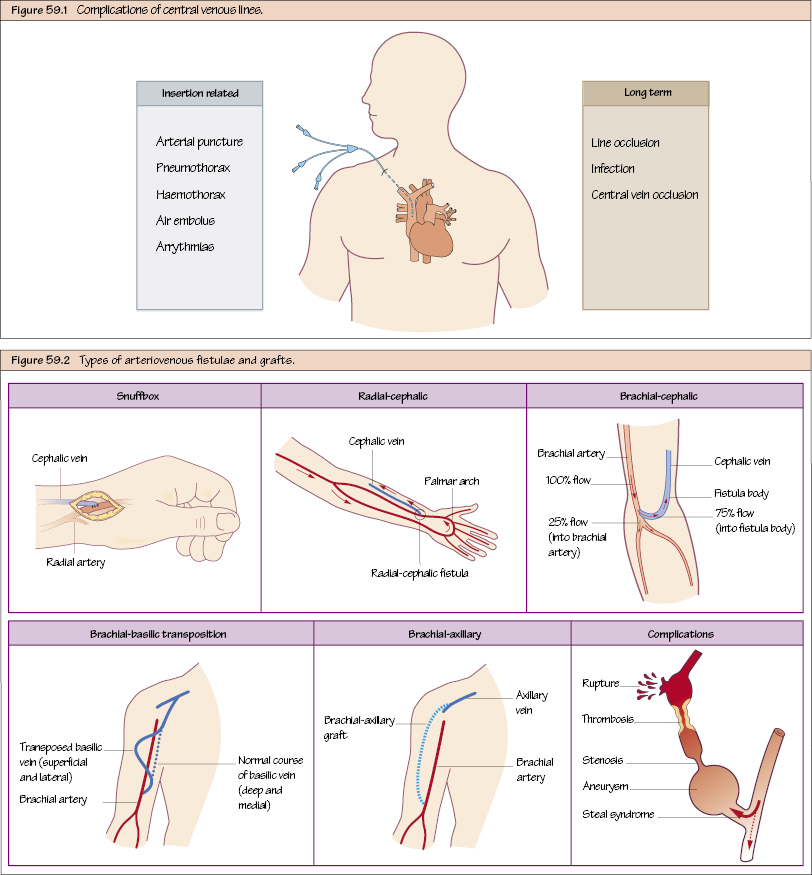
Principles of Fistula Creation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


