CHAPTER 1 General Setup and Techniques
Definition and Philosophy
A VATS procedure is not a compromise operation; it is the same operation that can be performed by a thoracotomy.1,2 The standard operation is performed with visualization on a monitor and through incisions without spreading the ribs. Procedures such as a video-assisted lobectomy provide the same complete cancer operation that is performed through a thoracotomy.3–12
Positioning
♦ For most VATS procedures, the patient is placed in the lateral decubitus position with a slight posterior tilt. The patient is taped in place. The arms are at 90 degrees, with the elbows bent in a praying position and with two pillows between the arms. Padding between the arm board and the downside elbow minimizes the risk of compression causing damage to the ulnar nerve.
♦ The operating table is flexed with the patient’s anterior-superior iliac crest positioned over the flexion of the table. This opens the rib spaces, and this position shifts the hip out of the way so it does not interfere with the movement of the thoracoscope.
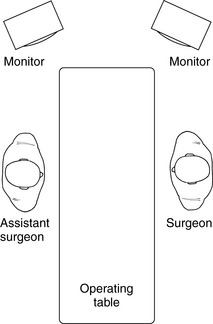
♦ The monitors are placed above the head of the operating table so that the surgeon and all assistants have an unobstructed view of the monitors (Figure 1-1). The surgeon stands on the anterior side of the patient.
♦ Different positioning may be used for other video-assisted thoracic operations. For example, a Heller myotomy is performed with the monitors at the foot of the bed.
Incisions
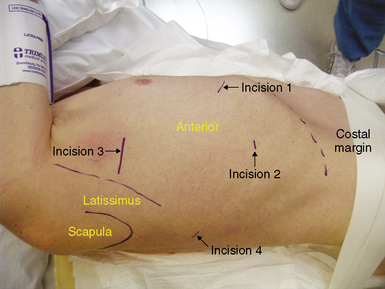
Placement of the incisions (Figure 1-2) is key to the performance of VATS. Proper placement of the incisions creates the best angles for the instruments to perform these procedures.
Incision 1
♦ Incision 1 is 2 cm long and placed in the intercostal space that is just below the inframammary crease. It is placed as far anteriorly and inferiorly as possible (approximately the sixth intercostal space in the midclavicular line).
♦ The incision through the chest wall is angled posteriorly so that it automatically directs instruments through this incision toward the major fissure and away from the pericardium.
♦ A finger through this incision confirms that there is no pleural symphysis. If one is detected, blunt dissection is performed to create a space for the trocar to pass through incision 2.
Incision 2
♦ It is placed low in the chest to provide a panoramic view of the chest. It is in the eighth intercostal space in the posterior axillary line.
Incision 3
♦ Incision 3 is a utility incision through which much of the dissection is performed and through which a lobe is removed.
♦ The location of the interspace for the incision is based on the superior pulmonary vein. Through incision 1, a ring forceps pushes the lung posteriorly to expose the superior pulmonary vein. Pressure on the chest wall helps to identify the interspace that is directly up from the vein. That space is used for an upper lobectomy, and one space lower is used for a middle or lower lobectomy.



