Despite intensive research efforts, the causative mechanisms of takotsubo cardiomyopathy (TC) are still unknown. Recently, morphologic characteristics of the left anterior descending coronary artery (LAD) have been proposed as a potential pathophysiological substrate. Hence, the aim of the present study was to evaluate the prevalence of myocardial bridging and LAD recurrent segments in a large cohort of patients with TC. A total of 161 patients with TC were matched for age and gender with 161 controls without coronary artery or valvular heart disease. Myocardial bridging was diagnosed according to indirect signs in coronary angiography. Furthermore, the LAD was evaluated regarding parts of the vessel outreaching the left ventricular apex (LAD recurrent segment). The prevalence of myocardial bridging was similar in the TC and control groups (11.8% vs 6.8%, p = 0.18). Any part of the LAD outreaching the left ventricular apex was observed in 55.6% of patients with TC compared with 35.4% in the control population (p <0.001). Moreover, the LAD supplied ≥25% of the inferior myocardial wall in 21 patients with TC (13.1%), whereas patients in the control group did not show this pattern of coronary circulation at all (p <0.001). Patients with TC with typical apical ballooning compared with those with atypical ballooning patterns demonstrated a higher prevalence of myocardial bridging (p = 0.04) but not LAD recurrent segments (p = 0.28). In conclusion, the prevalence of myocardial bridging in patients with TC is low and comparable with that in a matched control group. In contrast, LAD recurrent segments are significantly more frequent in patients with TC.
Despite intensive research efforts, the pathophysiology of takotsubo cardiomyopathy (TC) is still unknown. Recently, myocardial bridging of the left anterior descending coronary artery (LAD) was reported to be a frequent finding in patients with TC. Myocardial bridging is defined as an intramyocardial segment of an epicardial coronary artery. Although it is generally considered a normal variant, myocardial bridging has been linked to myocardial ischemia, myocardial infarction, and sudden death. Furthermore, a long LAD that outreaches the apex and supplies the inferior wall of the left ventricle (LAD recurrent segment or wraparound LAD) was observed in some TC cohorts. However, this has not been a consistent finding. In view of inconclusive data and the potential causative role of these morphologic characteristics of the LAD, the aim of the present study was to evaluate the frequency and significance of LAD recurrent segments and myocardial bridging in a large population of patients with TC.
Methods
This case-control study consisted of 161 consecutive patients with TC admitted to the University of Leipzig – Heart Center from January 2005 to June 2013. TC was diagnosed on the basis of the Mayo Clinic criteria in patients presenting with apparent symptoms of acute coronary syndrome: (1) transient left ventricular (LV) systolic dysfunction with typical regional wall motion abnormalities beyond the territory supplied by a single coronary artery, (2) absence of significant obstructive coronary artery disease or angiographic evidence of plaque rupture, (3) new electrocardiographic abnormalities (ST-segment elevation and/or T-wave inversion) or modest elevation of cardiac troponin levels, and (4) absence of pheochromocytoma and myocarditis. Additionally, the diagnosis was confirmed by cardiovascular magnetic resonance.
The TC cohort was matched for age (±3 years) and gender with 161 patients who underwent coronary angiography for suspected coronary artery disease from January 2013 and December 2013. They were recruited from the computerized medical records using a predefined query. Patients with significant (>50%) obstructive coronary artery disease or valvular heart disease were excluded.
All patients provided informed consent for the use of their records for research purpose. The study complied with the principles of the Declaration of Helsinki.
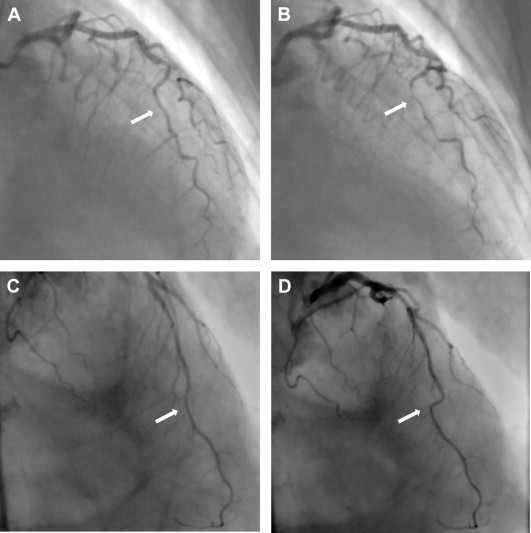
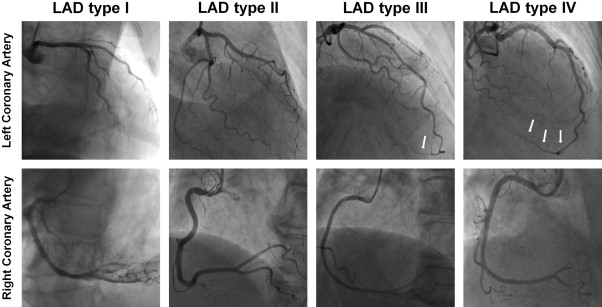
Coronary angiography had been performed in all patients using a transradial or transfemoral approach with a 5Fr or 6Fr catheter, and the LAD had been recorded in multiple views. The presence of significant obstructive coronary artery disease was evaluated visually. The coronary artery dominance was determined according to the supply of the posterior descending artery and the posterolateral branches. Myocardial bridging was diagnosed on the basis of the following indirect signs: (1) systolic compression of the LAD resulting in narrowing of the lumen that reverses during diastole, also called a “milking effect” ( Figure 1 ), and/or (2) the “step-down and step-up” phenomenon, defined as a localized change in the direction of the LAD’s course toward the ventricle and backward ( Figure 1 ). LAD recurrent segment (wraparound LAD) was defined as any part of the vessel outreaching the LV apex. The length of the recurrent segment was measured between the apical point of the LAD and the visible end of the coronary artery. Furthermore, LAD morphology was categorized in 4 types, similar to a previous investigation : type I, the LAD terminates before reaching the apex; type II, the LAD and the right coronary artery supply the apex; type III, the LAD supplies the entire apex; and type IV, the LAD supplies ≥25% of the inferior myocardial wall ( Figure 2 ). All images were analyzed by 2 experienced investigators blinded to study group and clinical data. Any disagreements were resolved by consensus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


