1 Fetal Circulation
II. OVERVIEW OF THE FETAL CIRCULATION
Fetal circulation is shown in Figure 1-1.

A. Oxygenation
1. Blood is oxygenated in the placenta.
2. Oxygenated blood returns to the fetus via the umbilical vein.
3. The umbilical vein courses into the hilum of the liver and joins the portal vein.
4. Umbilical venous blood is directed in part through the ductus venosus, which joins the inferior vena cava (IVC).
5. Oxygen-rich ductus venosus blood is preferentially directed into the left atrium and left heart through the foramen ovale.
6. Venous return of the left heart is composed of both ductus venosus and pulmonary venous blood.
7. The less-oxygenated blood of the liver (largely right lobe) and the superior vena cava (SVC) is directed into the right atrium and right heart.
B. Function
1. The left and right hearts function in parallel rather than in series. The left ventricle (LV) ejects largely to the coronary arteries and upper body with an arterial PaO2 (in fetal lambs) of 25 to 28 mm Hg. The right ventricle (RV) ejects largely to the lungs, the lower body, and the umbilical artery via the ductus arteriosus with an arterial PaO2 of 20 to 23 mm Hg (in fetal lambs).
2. With a high pulmonary vascular resistance, less than 20% of the cardiac output goes through the fetal lungs. This percentage increases in the third trimester.
3. The combined cardiac output of the fetal heart is 450 mL/kg per minute with increasing RV dominance through the second and third trimesters. In contrast, the combined output is 800 mL/kg per minute in the series circulation after birth.
III. THE PLACENTA
B. Function
1. The placenta provides nutrients and respiratory gas and metabolic exchange between the mother and fetus.
2. Uteroplacental flow increases during gestation in three phases as a result of vasodilation.
a. The first phase may occur within days or weeks of pregnancy.
b. The second phase occurs with development of intravillous spaces.
c. The third phase occurs during rapid fetal growth after 30 weeks. This corresponds with a change in uterine blood flow from less than 1% of the maternal cardiac output to 16% to 25% near term.
a. Complete fetoplacental circulation is established around the start of the fifth week after conception.
b. Fetoplacental blood flow, like uteroplacental flow, exponentially increases throughout gestation.
c. Placental blood volume is approximately 30% of the combined fetal cardiac output between 20 weeks and term.
a. In the first trimester, umbilical artery Doppler flow studies have demonstrated a gestational-age-dependent fall in placental resistance, with essentially no forward diastolic flow in the late first trimester.
b. In the second and third trimesters, Doppler flow studies indicate increasing flow velocities in diastole in keeping with the decreasing placental resistance.
IV. FETAL SHUNTS
A. Ductus venosus (Fig. 1-3)
1. The ductus venosus provides access for much of the highly oxygenated blood from the umbilical vein to the fetal IVC, which streams preferentially into the left atrium as a consequence of the IVC’s central position and relationship with the foramen ovale, septum primum, and septum secundum.
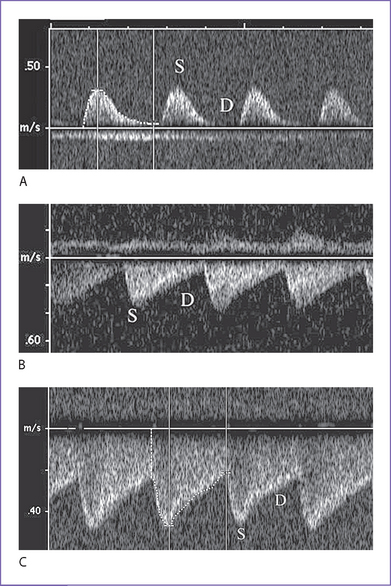
2. On Doppler flow interrogation in the fetus, the ductus venosus can be readily identified by the flow acceleration that occurs within its lumen.
a. It has the highest flow velocities observed in the systemic venous system.
b. Its pattern of flow is phasic but continuously antegrade, with the lowest velocity during atrial contraction.
3. Absence (or agenesis) of the ductus venosus.
a. The umbilical vein may connect with the portal venous system, another systemic vein such as the IVC, or the right atrium itself.
b. At least in the latter two conditions, a high cardiac output state often develops in the fetus, suggesting that the ductus venosus in some way regulates the umbilical venous return.
4. Ductus venosus patterns change in the context of evolving fetal heart failure. These suggest a protective mechanism that prevents modestly elevated central venous pressures from significantly influencing the critical umbilical venous return.
a. Flow patterns show gradual reduction in forward velocities during atrial systole in the ductus venosus.
b. Flow patterns show ultimate development of a wave reversal that usually occurs before the development of umbilical venous notching.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


