Familial Hyperlipidemia and Exertional Chest Pain
A 52-year-old woman with familial hyperlipidemia complains of exertional chest pain but walks 2 to 5 miles daily without difficulty. She is feeling depressed and has had weight gain.
She has a 12-lead electrocardiogram (ECG) as depicted in Figure 33-1 and undergoes a supine bicycle stress echocardiogram with imaging at rest (heart rate [HR] 52 beats per minute; Videos 33-1 and 33-2), at intermediate exercise (HR 90 beats per minute; Videos 33-3 and 33-4), and during peak stress (HR 131 beats per minute = 78% maximum predicted HR; Videos 33-5 and 33-6), end-systolic frames depicted. Left ventricular ejection fraction is normal at rest without wall motion abnormalities (Fig. 33-2).
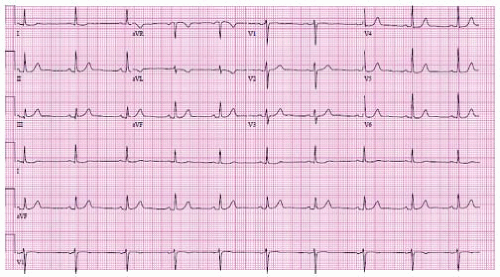 Figure 33-1. Resting 12-lead ECG. |
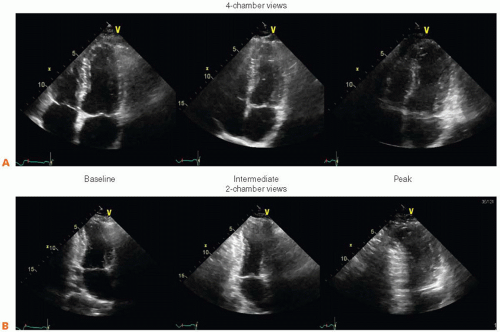 Figure 33-2A,B. |
QUESTION 1. Which statement is true?
A. The left ventricle (LV) is smallest at the intermediate stage exercise, suggesting a hibernating myocardium at rest
B. The LV cavity dilates at peak stress in a uniform pattern, suggesting a nonischemic cardiomyopathy
C. The LV cavity dilates in a regional pattern during peak stress, suggesting an ischemic response to stress
View Answer




ANSWER 1: C. It is correct that the LV is smallest during intermediate stage exercise. This is a normal response to exercise, and in a patient with normal LV systolic function to start does not imply a hibernating myocardium. Our patient has regional variation in myocardial contractility during peak stress (Fig. 33-4), consistent with obstructive coronary artery disease. A patient with global LV dilatation at stress may have a nonischemic cardiomyopathy, significant valvular disease, or may have ischemic disease due to left main or triple vessel disease.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
