Cardiac specimens may be procured for examination either at autopsy or surgery. Autopsy-derived specimens are in the context of a forensic (legal) investigation or a medical procedure (so-called hospital autopsy). Surgical specimens are removed in the course of biopsy, excision, repair, or replacement of diseased cardiovascular tissue and may be in the form of biopsies, valve resections or repairs, myectomies, repairs of congenital heart disease, explants, and other procedures.
Regardless of the setting in which cardiac tissue is to be examined, there are common principles that should be kept in mind prior to handling and/or processing. First and foremost, a thorough understanding of the clinical situation in which the tissue was procured is essential. The documentation, dissection, tissue processing, and reporting will all be contingent upon the clinical scenario. In this chapter and those that follow, emphasis is placed on how to handle and evaluate specimens in the context of different circumstances. Second, documentation of the examination and handling is necessary throughout the process and ideally includes both thorough written description as well as liberal photography. Finally, a uniform approach to documentation is strongly encouraged for consistency and efficiency.
Cardiac Examination at Autopsy
General Considerations
Autopsy-derived cardiovascular specimens may be evaluated in the context of either a forensic or medical autopsy. In the case of forensic evaluation, the objective is primarily to determine cause and manner of death. In establishing a natural manner of death, it is important to exclude noncardiac causes as the heart may be grossly and microscopically normal in cases of sudden arrhythmic death (see Chapter 141). Conversely, it is also important to keep in mind that arrhythmic substrates may exist in individuals who die of noncardiac causes.
TABLE 138.1 Goals of Cardiac Evaluation at Autopsy
Forensic autopsy
Establish the manner of death (natural, accident, homicide, suicide)
Identify a natural cardiac cause if extracardiac and unnatural causes have been excluded
Identify the cause as unexplained arrhythmia in the absence of significant cardiac and extracardiac findings (see Chapter 141)
Medical autopsy (and to a lesser extent forensic autopsies)
Document cardiac pathology, including iatrogenic
Correlate cardiac findings with history and interventions
Determine a cardiac or noncardiac cause of death
Determine possible contributing cardiac causes of death
Preserve the specimen after proper dissection and diagnosis, if allowed in the autopsy permit, for a reasonable period of time for potential subsequent investigations
Perform postmortem radiographs in cases of stents or prosthesis, when indicated
Photograph the specimen as necessary
Medical (nonforensic) autopsies may be performed for a number of reasons. Like their forensic counterparts, they also may be performed to more definitively establish a cause of death (though the manner is almost invariably natural). They also may be performed to document pathology and interventions (including potential complications thereof) (Table 138.1).
In either forensic or medical autopsy, it may be important to preserve tissue for molecular study, especially in the setting of sudden death (see Chapter 141). Such can typically be best accomplished by reserving whole blood in an EDTA (lavender top) tube until the autopsy is completed. Increasingly, paraffin samples can be utilized to answer many questions with newer-generation nucleic acid sequencing techniques.
Whether dealing with a forensic or medical autopsy, appropriate evaluation of the patient history and medical record is paramount. Information contained in the history will help to guide the examination, documentation, and handling. Important facts to know prior to autopsy include changes in circulatory status (abrupt or gradual), cardiac rhythms, and cardiac interventions. An example of a handout to be completed prior to autopsy is illustrated in Table 138.2.
Finally, the method of dissection and evaluation described below is a general dissection method. Although nearly all varieties of congenital and acquired heart disease can be evaluated and documented using this method, other dissection techniques (such as dissecting along tomographic planes or base-of-the heart dissections) can be of utility in certain circumstances.
TABLE 138.2 Worksheet for Preautopsy Preparation
Date of admission _______________________________________________________
Date of admission at outside facility (if transferred) ___________________________
Major problem at admission ______________________________________________
Date of death and time interval between admission and death: ___________________________________________________________________
Recent medical history (cause for admission):______________________________________________________
Important prior medical and surgical historya:______________________________________________________ ________________________________________________________________
Hospital course, surgical interventions, and dates, including complications: _________________________________________________________________________ _________________________________________________________________________ _________________________________________________________________________
Hospital course, medical complications, and dates: _________________________ ___________________________________________________________________________ _________________________________________________________________________ _________________________________________________________________________ _________________________________________________________________________
Circumstances of deathb:________________________________________________
Presumed cause of death (clinical): __________________________________________
Questions to be answered: __________________________________________________ _________________________________________________________________________
aPrior cardiac operative notes are very helpful. If not immediately available, they can be accessed after autopsy and before cardiac dissection, which generally occurs after proper fixation.
bFor example, hypotensive shock, hemorrhage, septic shock, cardiogenic shock, shock of unclear etiology; sudden death (witness or not), cardiac arrest, respiratory arrest, cardiorespiratory arrest or arrest of uncertain etiology; brain death with removal of life support.
Removal of the Heart at Autopsy
The examination of the adult heart begins after the anterior chest plate has been removed. The pericardium is inspected for effusions (abnormal amounts of fluid; normal <50 mL of straw-colored fluid) or blood, and the amount of pericardial fluid is measured. The surface of the visceral as well as parietal pericardium is also examined for exudates, adhesions, tumor nodules, or other lesions. The heart can then be removed from the thorax, or the heart and lungs can be removed en bloc. The latter approach is described as it allows the removal of the abdominal viscera to proceed while the thoracic block is being evaluated. The superior and inferior venae cavae should be cut leaving ˜1 cm of each on the thoracic block. The aortic arch vessels should likewise be cut ˜1 cm from their origins. Transection of the esophagus and trachea can proceed at the level of the thoracic inlet. At this point, reflection of the block from superior to inferior can proceed, using scissors to separate the periaortic tissue from the vertebral bodies. The esophagus may be tied off at the diaphragmatic crux and then transected distally as well.
Once the thoracic block is removed, a posterior approach is recommended to begin separation of the pulmonary venous connections. First, the esophagus is reflected upward and removed. In fetal autopsies, careful evaluation for a tracheoesophageal fistula is warranted (usually by first opening the esophagus posteriorly and visually inspecting the anterior luminal surface). Next, the posterior parietal pericardium is incised from the inferior edge up to the carina, effectively dividing it into left and right portions. Reflecting these respective portions will reveal the pulmonary venous drainage that typically includes a right-sided upper and lower pulmonary vein as well as a left-sided upper and lower pulmonary vein. Blunt dissection of the pericardium around these veins will enable the prosector to leave 1 cm of each vein attached to the left atrium.
After the pulmonary veins have been separated, the block may be turned over and approached from the anterior aspect. Excess anterior parietal pericardium may be removed at this time. The pulmonary artery should be transected ˜1 cm above the infundibulum, and the aorta should be transected just beyond the sinotubular junction. It is important to keep in mind that the ascending aorta and main pulmonary artery are nearly perpendicular to one another, with the former directed toward the right shoulder and the latter directed toward the left shoulder. Thus, the cuts should be made at nearly 90 degrees with respect to one another to achieve perfect cross sections. The superior vena cava can then be reflected anteriorly and inferiorly.
At this point, the only connection the heart will have to the thoracic block is through a fold of fibroadipose tissue situated just inferior to right and left pulmonary arteries. Hence, careful separation just beneath the pulmonary bifurcation will effectively separate the heart from the rest of the thoracic block. The main pulmonary artery and branches can then be dissected with the lungs, including evaluation for pulmonary embolism.
Depending on the clinical/forensic questions to be addressed, it may be useful to fix the heart (by perfusion or otherwise) at this point for a specific dissection and/or consultation. Such perfusion may be achieved by placing the heart several feet below a formalin source. The aorta, one of the vena cava, and one of the pulmonary veins can be cannulated with clamps, tubes, and/or glass cannulas. All remaining vascular connections can be tied off. Simple perfusion for 20 minutes, followed by formalin submersion, will often allow adequate fixation. If such perfusion is not possible, a short-axis cut at the midventricular level, parallel to the cardiac base (dividing the heart into apical and basal halves), will usually allow for adequate fixation of the external and internal structures.
External Examination and Weighing the Heart
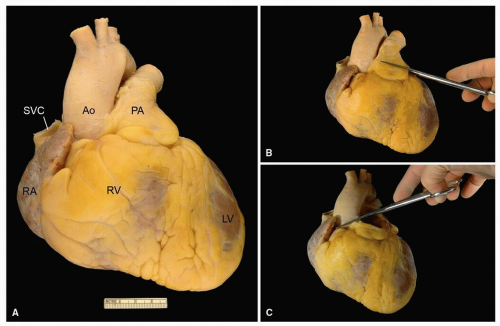
Following separation of the heart from the thoracic block (and fixation, if performed) (Fig. 138.1A), the remaining great arteries may be trimmed from the heart (˜1 cm above the semilunar valves) (Fig. 138.1B, C). The great arteries are positioned ˜60 to 90 degrees relative to one another, necessitating cuts in different planes. After removal of the great arteries, the heart should be weighed. The heart should be free of postmortem clot, and gentle manual removal through the venae cavae or pulmonary veins is usually adequate. The presence of a large or firm clot within the heart may necessitate reweighing the heart after dissection.
FIGURE 138.1 ▲ A. External, anterior, view of the heart procured at the time of autopsy. From this perspective, the following structures can be readily identified: right atrium (RA), right ventricle (RV), left ventricle (LV), superior vena cava (SVC), ascending aorta (Ao), and the main pulmonary artery (PA). B. Transection of the pulmonary artery, ˜1 cm above the pulmonary valve commissures. C. Transection of the ascending aorta, ˜1 cm above the aortic valve.
Heart weight should be compared to standard nomograms, given the individuals body size.1,2 In general, body weight is a better correlate with heart weight than height, unless the decedent is morbidly obese or cachectic. As a rule of thumb, male heart weight is ˜0.45% of body weight and female heart weight is ˜0.4% of body weight.3,4
Heart weight is the single best indicator of cardiac hypertrophy. After weighing, the external surfaces of the heart should be inspected and described. The epicardial surface should be smooth and glistening.
Examination of the Coronary Arteries
In general, the epicardial coronary arteries are best evaluated after removal from the heart and decalcification (depending on the firmness of the vessels themselves). Radiographic evaluation of the heart specimen can help in the determination of the extent of coronary calcification, as well as calcification in other areas of the heart (Fig. 138.2). Such radiographic evaluation can also be useful in the identification and localization of intravascular stents or other intracardiac hardware.
The epicardial course should be described along with the dominance pattern (Fig. 138.3). Approximately 70% of hearts will exhibit right dominance, in which the posterior descending coronary artery is derived from the right coronary artery. About 20% of the time, the posterior descending coronary artery is derived from the left circumflex coronary artery, with the balance consisting of those that exhibit shared (derived from a combination of right coronary and left circumflex coronary arteries) dominance. The coronary arteries are best handled after removal from the heart (Fig. 138.4).
Only gold members can continue reading. Log In or Register to continue