Chapter 13
Endomyocardial Biopsy
1. Why is an endomyocardial biopsy (EMB) performed?
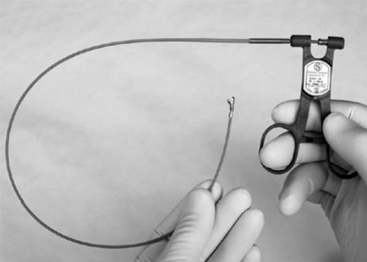
A bioptome is shown in Figure 13-1. The Stanford-Caves-Schultz and the King bioptomes access the right ventricle through the right internal jugular vein. A modified Cordis bioptome (B-18110, Wolfgang Meiners Medizintechnik, Monheim, Germany) has been used for access from the right femoral vein. The subclavian and left femoral veins are used less frequently.
The femoral artery may be used as a percutaneous access site for left ventricular biopsy.
3. What are the risks associated with an EMB?
Risks correlated with EMB are summarized in Table 13-1. EMB is associated with a serious acute complication rate of less than 1% using the current flexible bioptomes, and the overall rate of complication is reported as less than 6% in most case series. Complications include access-site hematoma, transient right bundle branch block (RBBB), transient arrhythmias, tricuspid regurgitation, and, rarely, pulmonary embolism. Life-threatening complications occur far less frequently. Right ventricular perforation was reported in less than 1% of patients. Following cardiac transplant, the risk is especially low. The risks of EMB depend on the clinical state of the patient, the experience of the operator, and site procedural volume.






