3
Emissions related to cooking and heating
In most developed nations the majority of households cook and heat their homes with either electricity or natural gas. Wood, coal, peat, kerosene and town gas have been popular fuels in the not so distant past and remain the preferred option for some modern day householders. The use of each of these fuels in the home, except for electricity, has been reported to be associated with respiratory morbidity in children and adults in different parts of the world.
In the less developed parts of the world, biomass remains a dominant indoor fuel source. Some have estimated that more than half the world’s population still relies on unprocessed biomass fuels (wood, crop residues and dung cakes) that are burnt in poorly ventilated homes using simple pits or rudimentary mud-formed cooking stoves. Emissions from these sources are recognized as a major cause of acute and chronic respiratory morbidity in children and adults living in these homes and are a major international public health concern. The World Health Organization is leading an international effort to reduce the health effects of biomass fuel usage.
Regardless of what fuel is being burnt, exposure to the pollutants produced will vary with the amount of time spent in the affected area (which may depend on gender, climate or other socio-economic or cultural factors) and ventilation of the area (which may depend on local housing regulations, climate and cultural housing norms). These variations are likely to contribute to the inconsistent findings from research studies that have examined the association of health with exposure to pollutants from heating and cooking in the developed world. Although an association of a range of respiratory conditions with indoor pollution from cooking or heating is suspected, further evidence is needed before a causal association can be proven. This is particularly the case for the health effects of the use of gas cooking and gas heating appliances and poses a dilemma for clinicians in developed nations. What should they say to patients who have respiratory complaints and who use indoor gas heating appliances? Should they advise a switch to electrical appliances? Furthermore, in the developed world, there has recently been a growth in the use of wood burning stoves. It is uncertain whether modern wood burning appliances may also be associated with increased indoor pollution and disease.
The aim of this chapter is to provide a summary of current knowledge of the respiratory health effects of fuels used for heating and cooking, highlighting areas of certainty and areas of doubt. I will focus predominantly on the current modern day dilemma – whether to use gas or electricity – but will mention where relevant other common indoor fuels used in the developed nations.
The proportion of the population which uses gas for cooking and heating varies across the world. A main natural gas supply is absent in some countries (e.g. Norway), in some parts of some countries (e.g. rural areas) and in some types of housing stock (e.g. in modern blocks of flats). Where natural gas is absent, bottled gas may be available, stored either outside the home in large tanks or inside the home in bottles. The most common alternative fuel is electricity, but other fossil fuels such as kerosene, paraffin, coal, oil and peat as well as wood may be used, depending on local supply and local practice. All of these fossil fuels have one thing in common – as they combust, a range of gases and particulates are produced which may be harmful to respiratory health. Occupants of homes using these fuels will have higher exposure to pollutants if the appliance is faulty, the flue is blocked or the rooms in which they are used are poorly ventilated
3.3 Pollutants produced when using gas appliances in the home
Combustion of fossil fuels and biomass in the home produces gases such as nitrogen dioxide, carbon monoxide, particles and other potentially toxic substances such as formaldehyde, volatile organic compounds and sulfur dioxide. We know much more about exposure to nitrogen dioxide in the home than most of the other pollutants. This is because relatively cheap and reliable passive samplers are available for measuring average levels of indoor nitrogen dioxide and have been used in large-scale studies. Because pollutants (including nitrogen dioxide) from fossil fuel combustion are present in the outdoor air, a proportion of the indoor levels may come from the outside, the proportion depending on the relative balance of indoor and outdoor sources.
The combustion of gas at high temperatures produces nitric oxide, which is oxidized to nitrogen dioxide, and other oxides of nitrogen including nitrous acid. Indoor nitric oxide levels, which are rarely measured, are usually low, although some experimental studies suggest they reach higher levels in poorly ventilated conditions. On the other hand, when a gas oven or hob is turned on, there is a sharp rise in nitrogen dioxide level, which diminishes slightly as the appliance heats up and gas burning becomes more efficient. High levels are maintained until the appliance is turned off and this is followed by a steady decay that depends largely, but not exclusively, on ventilation of the kitchen and circulation of air from the kitchen to other parts of the house.
In studies that have continuously monitored nitrogen dioxide levels in areas near a gas cooker in use. the peaks measured have been recorded to be as high as 1100 μg/m3 (USA, late 1980s), 2500 μg/m3 (USA, late 1990s) and 3000 μg/m3 (UK, late 1980s). These values are far higher than those recorded by continuous monitoring of ambient air as part of the outdoor pollution monitoring programme in the UK and far higher than the World Health Organization’s short-term hourly guideline value for nitrogen dioxide in ambient air of 200 μg/m3.
These peaks of exposure are rarely measured in large-scale health studies as continuous monitoring of indoor nitrogen dioxide involves cumbersome and expensive equipment. Passive sampling over a one to two week period generates an average value only and masks the peak levels that may have occurred. Some have argued that the use of passive samplers to quantify exposure to indoor nitrogen dioxide is unlikely to aid assessment of health effects of the use of gas appliances because of this problem and that all is needed is knowledge of the main types of fuel used in the homes.
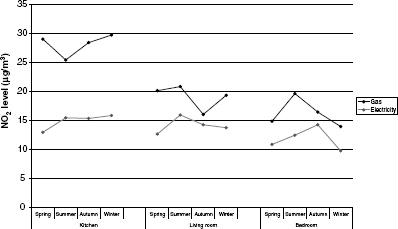
The use of gas for cooking increases not only the average kitchen level of nitrogen dioxide but also the average levels in other rooms (Figure 3.1) particularly if doors are left open between the kitchen and the rest of the house.
Figure 3.1 Mean measured nitrogen dioxide level (μg/m3) in kitchen, living room and bedroom in English homes that use gas or electricity for cooking (drawn from data presented in: Berry et al. [1])
There is some evidence that homes with gas ovens have higher nitrogen dioxide levels than those that only have gas hobs (or ranges). Indoor kitchen levels will be higher if there is a pilot light on the gas cooker, but this is not a common feature of gas cookers currently produced. It is not clear whether the use of particular types of gas (e.g. bottled gas) causes higher levels of nitrogen dioxide than the use of natural gas, although some studies in some parts of the world suggest this is the case.
There are marked seasonal differences in indoor nitrogen dioxide level in homes that use gas, with lower levels in summer when windows and doors are more likely to be open to cool and ventilate the home. Summer is a time when less cooking is done and more cold food is eaten, so usage of gas ovens as well as gas heaters is less common, leading to lower levels of indoor pollutants.
Kitchen ventilation by the use of ‘active aspiration devices’ has been found in some reports to be associated with lower levels of kitchen nitrogen dioxide when gas cookers are present, but this is not always the case. Indeed the most effective means of ventilating a kitchen is to open a door or window to the outside air, which should lead to much lower levels of all combustion pollutants in the kitchen.
Nitrous acid (HONO) is present as a gas in indoor and outdoor air. In the indoor environment nitrous acid is produced both directly by gas combustion and indirectly by absorption of nitrogen dioxide and then release of nitrous acid from water-containing surfaces in the home. Nitrous acid levels in the outdoor air are substantially lower than indoor levels due to rapid photodissociation in sunlight and therefore indoor levels are a result of indoor combustion processes.
Nitrous acid will interfere with accurate measurement of nitrogen dioxide by the most commonly used passive samplers. Some have suggested that the actual measured nitrogen dioxide level from these samplers should be ‘adjusted’ or ‘corrected’ for this interference. More importantly it has been proposed that adverse health outcomes that have been attributed to nitrogen dioxide (or to exposure to nitrogen dioxide-producing appliances such as gas stoves) could be confounded (or explained) by exposure to nitrous acid. It has been argued that the inconsistent results from studies that examine the association of indoor nitrogen dioxide with respiratory health may be explained by failure to measure this co-pollutant. Nitrous acid can be measured by a passive sampler but there is a dearth of studies in which both nitrous acid and nitrogen dioxide have been measured.
As for indoor nitrogen dioxide, indoor nitrous acid levels are higher in gas-cooking homes, likely to be higher in homes with gas ovens rather than just gas hobs and follow a seasonal pattern.
The act of cooking, particularly frying and the cooking of fatty foods, generates particles in the kitchen irrespective of the fuel used for cooking. However even if account is taken of this, the generation of particles when boiling water, stir frying, bacon frying, cake baking, meat roasting and potato baking produces higher peak concentrations of ultrafine particles if conducted with a gas, rather than electric, appliance. A prolonged peak of ultrafine particles has been shown to be generated by cooking potatoes in a gas oven for 75 min, but the peaks decay, possibly due to particles coagulating into large conglomerates after release.
Particles are generated by the use of a gas or electric cooker even if no cooking occurs. The particles generated by gas are smaller (15-40 nm diameter) than those generated by electric appliances, and are probably carbonaceous. There is very limited information available on the indoor particulate level that can be attributed to the use of gas for cooking or gas heaters and, as indoor particulate levels in living rooms and bedrooms are very much higher in homes with smokers, the public health effort has been directed towards this. In addition, concerns over penetration of outdoor particles generated by motor vehicles into the indoor environment has focused attention on this aspect of indoor particulate matter. However other fuels, such as wood and especially biomass, are likely to produce very high particulate levels in the indoor environment if not properly ventilated.
Gas combustion produces water vapour, which can lead to high levels of humidity in homes. High humidity encourages the growth of house dust mites, molds and bacteria within the home.
Combustion of natural gas and other fossil fuels will produce small quantities of formaldehyde, but the contribution of combustion sources probably adds only small amounts of formaldehyde in comparison to other indoor sources such as cosmetics, paints, coatings and insulation materials.
Sulfur dioxide is produced by fossil fuel combustion, particularly the burning of oil and coal, but indoor sources are thought to contribute little to overall exposure to this gas.
3.3.7 Total personal exposure vs indoor levels
Exposure to some of the pollutants produced by gas may occur in the outdoor environment due to other sources. Total personal exposure to nitrogen dioxide can be measured using passive samplers designed as badges to be clipped onto clothing and will depend on several factors including time activity patterns, ambient nitrogen dioxide levels and indoor nitrogen dioxide levels. For individuals who spend the majority of the day in the home, such as small children, housewives and the elderly, indoor sources are likely to be more important. In school children in the south of England, total nitrogen dioxide exposure was higher in those with a gas cooker or a pilot light on the gas cooker, those who lived with one or more smokers, and those who travelled to school by means other than a car. However these factors did not explain all of the variation in total personal exposure to nitrogen dioxide and the authors concluded that total personal exposure could only be determined by making direct measures and could not be imputed from questionnaire-derived information.
In the absence of indoor gas appliances, outdoor levels of nitrogen dioxide, which can show marked variation between homes in a single geographic area depending on the levels of outdoor traffic, is the most important determinant of total personal exposure to nitrogen dioxide.
3.4 Diseases associated with exposures
Respiratory morbidity has been associated with the use of gas appliances and levels of indoor nitrogen dioxide, but at present most would agree that there is insufficient evidence to confidently state that the reported associations are causal. Longitudinal studies, in which exposure is assessed prior to the development of disease, provide stronger evidence for casual links and some have shown health effects. However there are few randomized controlled trials that show whether reduction in exposure to gas appliances or indoor nitrogen dioxide leads to improvement in respiratory health. Many of the published cross-sectional studies have been criticized for inadequate adjustment for other household or socio-economic factors that may be important in disease aetiology and associated with high levels of gas use (confounders), and for failing to separate inception of disease from aggravation of existing disease. There are also concerns that many studies that have collected data and shown there is no association remain unpublished (publication bias).
While recognizing these caveats, there is a considerable amount of information from laboratory studies, chamber exposure studies and epidemiological studies that support the hypothesis that exposure to gas appliances and pollutants from combustion of other fossil fuels is harmful to respiratory health. The following patterns of respiratory illness have been suggested to be important:
(1) airway inflammation that is possibly related to oxidative damage and which may lead to symptoms of wheeze, cough and decrements in lung function;
(2) increased susceptibility to airway infections, particularly in small children, that may lead to increased reports of lower respiratory tract symptoms such as cough and wheeze;
(3) enhanced responses to inhaled allergen that are manifested as increased reporting of symptoms of cough and wheeze.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


