Fig. 15.1
A 16-year-old patient with disabling left varicocele, at rest and with effort, from several months. Renal ultrasound has eliminated any suspicious obstacle to the venous flow. A spermatic venography was requested, in order to perform an embolization if possible. (a, b) Right femoral vein puncture and catheterization of the left gonadal vein via the left renal vein: no obstacle or valvula was encountered in the path of the guidewire. Injection of 8 cc of ICM (4 cc/s), at the lumbar floor, and then at the pelvic floor. A unique gonadal vein drains into the renal vein, but in the pelvis the gonadal efferent branches are multiple, with two main trunks. (c) Control (manual injection by micro-catheter) after occlusion of both main efferent branches by micro-coils in the pelvis. (d) Additional lumbar occlusion a few centimeters higher, using an Amplatzer occluder plug (arrow). Control injection at the ostium of the gonadal vein, with reflux in the renal vein and the inferior vena cava
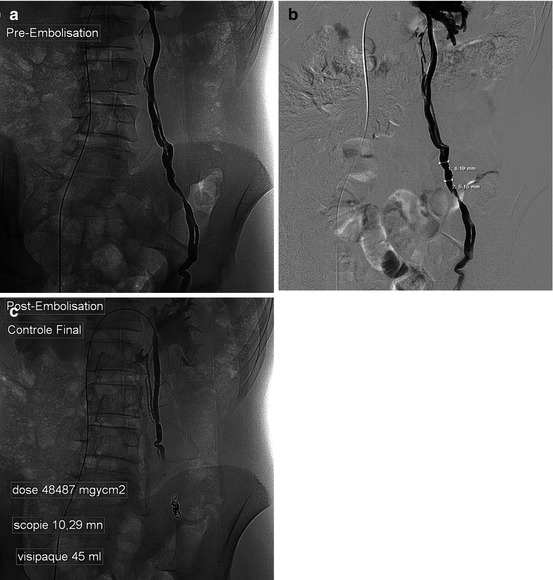
Fig. 15.2
Left varicocele which is very symptomatic on exercise (running) in a young 18-year-old. (a) After femoral vein puncture, catheterization of the left renal vein and of the spermatic vein, automatic injection (10 cc at 4 cc/s) in the left genital vein: the gonadal venous drainage is doubled in the pelvic and lumbar floors, but an apparently unique segment was shown in the iliac fossa, at which level we decided to perform the occlusion. (b) Sizing of the diameter of the repleted vein downstream of the target segment. To choose the coils, we performed a 10–20 % oversizing: coils of 7 and then 6 and 5 mm diameter were chosen. (c) Control after occlusion by coils
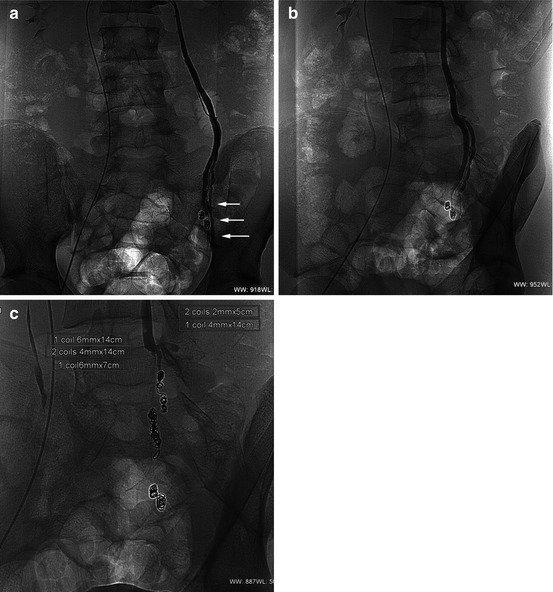
Fig. 15.3




A 18-year-old male; a recurrent symptomatic varicocele has already been surgically operated 3 years earlier; a first embolization has been then performed a few months after this surgery. (a, b: frontal and 37° LAO) Selective catheterization at the ostium of the left gonadal vein. The low pressure (4 cc/s) retrograde opacification showed a patent left gonadal vein (arrow), independent of the previously placed coils. This was probably due to the development of vicariances which were not visible on the first angiographic procedure. (c) After selective catheterization, the two main efferent branches have been occluded by calibrated coil packs. The manual control injection shows an effective occlusion
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
