Fig. 16.1
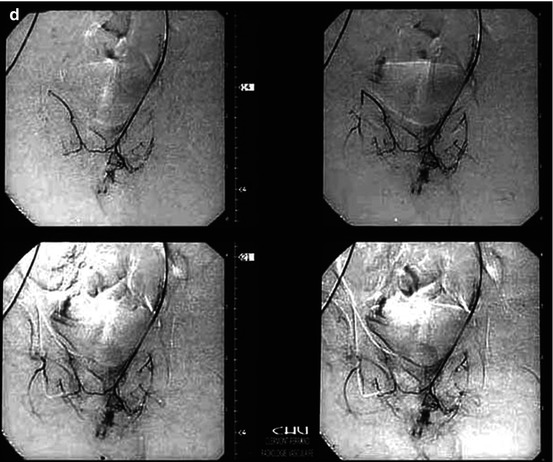
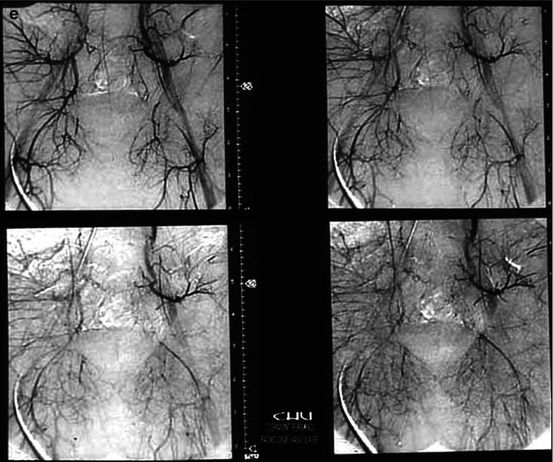
A 12-year-old patient, sustained priapism lasting for 3 days after falling astride on a bar. (a) Aortography (injection at the aortoiliac bifurcation): contrast extravasation at the root of the penis. (b) Hyperselective catheterization (4 F Cobra catheter): extravasation involving the right internal pudendal artery that was embolized using gelfoam (resorbable gelatin). (c) Control aortography: persistent extravasation at the root of the penis. (d) Selective catheterization of the left hypogastric artery from a right femoral puncture (crossover), followed by a hyperselective catheterization of the left internal pudendal artery. This artery also contributed to the traumatic cavernous fistula and was also embolized with gelfoam. (e) Aortographic final control: exclusion of the fistula
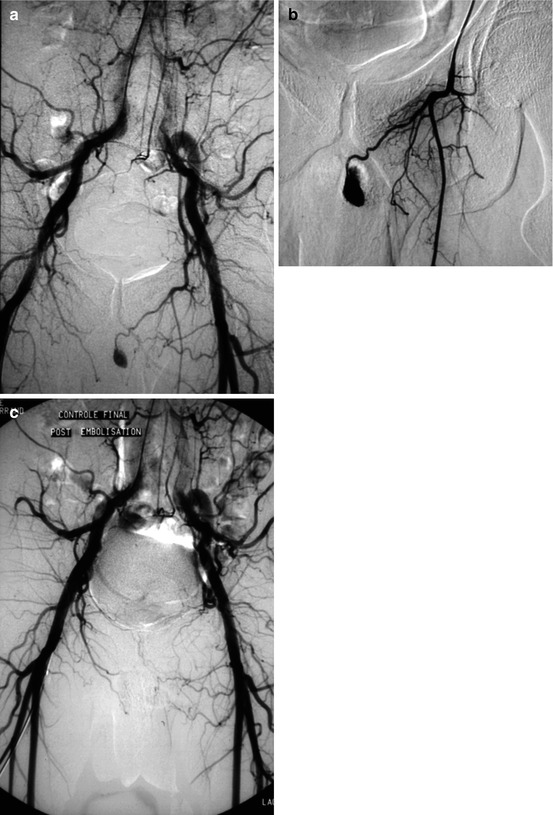
Fig. 16.2




A 25-year-old, highway motorcycle accident: isolated priapism 2 hours later (without any bony traumatic lesion). (a) Aortography. Intracavernous extravasation: a left internal pudendal arterial source of the extravasation was suspected. (b) From a right femoral artery puncture, a selective catheterization of the left hypogastric artery was performed: it confirmed a significant arterio-cavernous fistula, fed by the left internal pudendal artery. (c) Aortographic control (late phase) after embolization of the left internal pudendal artery with resorbable gelatin. Normal erections 1 month later
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
