The subcutaneous implantable cardioverter-defibrillator (S-ICD) represents an important alternative to traditional ICD therapy. The major limitation of this technology is the inability to provide pacing. Here, we present a case of a patient with complete heart block and a pacemaker who underwent placement of an S-ICD. Special considerations had to be taken with regards to evaluation and implantation of the S-ICD because of the pacemaker. In conclusion, implantation of an S-ICD can be done in patients with pacemaker effectively with appropriate electrocardiographic screening, device testing, and programming.
Case Description
A 58-year-old man was referred for an implantable cardioverter-defibrillator (ICD). He had a renal transplant before 10 years. Before his transplant, he received a right-sided dual chamber pacemaker with an atrioventricular junction ablation for atrial arrhythmias. The pacemaker was right sided as he had an atrioventricular fistula in the left arm. His renal transplant began to fail a year ago, and a new fistula was created in the left arm for dialysis. He is being worked up again for transplantation. Recent echocardiogram showed worsened left ventricular function.
Evaluation in our clinic demonstrated normal pacemaker function with underlying complete heart block. Several episodes of nonsustained ventricular tachycardia were recorded. Repeat echocardiogram confirmed severe left ventricular dysfunction. Venogram of the right shoulder showed significant stenosis of the innominate vein. Options were reviewed with the patient. These included upgrading the pacemaker to a biventricular ICD. This would require venoplasty or extraction of the ventricular pacing lead to gain vascular access. Another option would be to leave the right-sided system in situ and place a subcutaneous ICD (S-ICD). The transplant service requested we not use the left side because of his maturing fistula. Because of infection concerns, the patient elected to have an S-ICD.
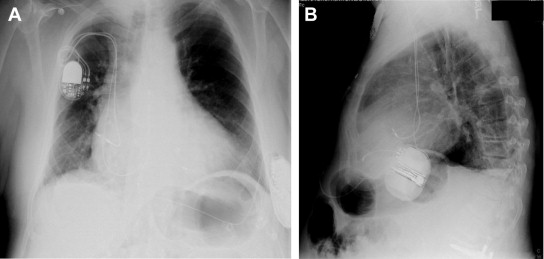
He underwent screening with the electrocardiographic screening tool, which was developed to evaluate for the risk of T wave oversensing by the S-ICD. The patient did not screen in because of large T-wave amplitude ( Figure 1 ). As the patient has complete heart block, it was believed that we could safely implant an S-ICD without risk of inappropriate shocks due to T wave double counting as long as the detection rate was >2X the upper rate limit of the pacemaker. The device was placed successfully ( Figure 2 ). Defibrillation testing was performed, and the patient successfully sensed and converted the episode. Pacemaker output was increased to maximum to look for marking of the pacemaker spike. During testing, the pacemaker was programmed to an asynchronous pacing mode at maximum outputs to ensure that the device would not interpret the pacer spikes as a normal rhythm ( Figure 3 ). At the end, the pacemaker was programmed to DDDR mode with an upper rate limit of 110 beats/min. The S-ICD was programmed to a detection rate of 230 beats/min with the conditional zone and postshock pacing off.