Emerging evidence suggests that endurance exercise increases the risk for atrial fibrillation (AF) in men, but few studies have investigated the dose-response relation between exercise and risk for atrial arrhythmias. Both exposure to exercise and reference points vary among studies, and previous studies have not differentiated between AF and atrial flutter. The aim of this study was to assess the risk for atrial arrhythmias by cumulative years of regular endurance exercise in men. To cover the range from physical inactivity to long-term endurance exercise, the study sample in this retrospective cohort study was based on 2 distinct cohorts: male participants in a long-distance cross-country ski race and men from the general population, in total 3,545 men aged ≥53 years. Arrhythmia diagnoses were validated by electrocardiograms during review of medical records. Regular endurance exercise was self-reported by questionnaire. A broad range of confounding factors was available for adjustment. The adjusted odds ratios per 10 years of regular endurance exercise were 1.16 (95% confidence interval 1.06 to 1.29) for AF and 1.42 (95% confidence interval 1.20 to 1.69) for atrial flutter. In stratified analyses, the associations were significant in cross-country skiers and in men from the general population. In conclusion, cumulative years of regular endurance exercise were associated with a gradually increased risk for AF and atrial flutter.
Highlights
- •
Long-term endurance exercise increased the risk for both AF and atrial flutter.
- •
Years of regular endurance exercise increased the risk for atrial arrhythmias gradually.
- •
Atrial arrhythmia diagnoses were validated by electrocardiography.
- •
The associations were consistent between cross-country skiers and men from the general population.
- •
The results were robust after adjustments for a broad range of confounding factors.
Emerging evidence suggests an exercise-induced excess in the incidence of atrial fibrillation (AF) in men, but few studies have investigated effects of long-term regular endurance exercise, and a dose-response relation between exercise and the risk for atrial arrhythmias remains to be determined. Moderate physical activity (PA) reduces the risk for AF in older adults, probably mediated thorough the beneficial effect on risk factors for AF such as heart disease, hypertension, and diabetes mellitus. In contrast, endurance sport participation seems to be an independent risk factor for AF in men aged ≥65 years. The aim of this study was to assess the dose-response relation between cumulative years of endurance exercise and risk for atrial arrhythmias in men aged ≥53 years.
Methods
To cover the range from physical inactivity to long-term regular endurance exercise, the study sample was based on participants recruited from 2 independent cohorts. Altogether, 4,999 men aged 53 to 92 years were invited to participate. Figure 1 illustrates the recruitment to this retrospective cohort study.
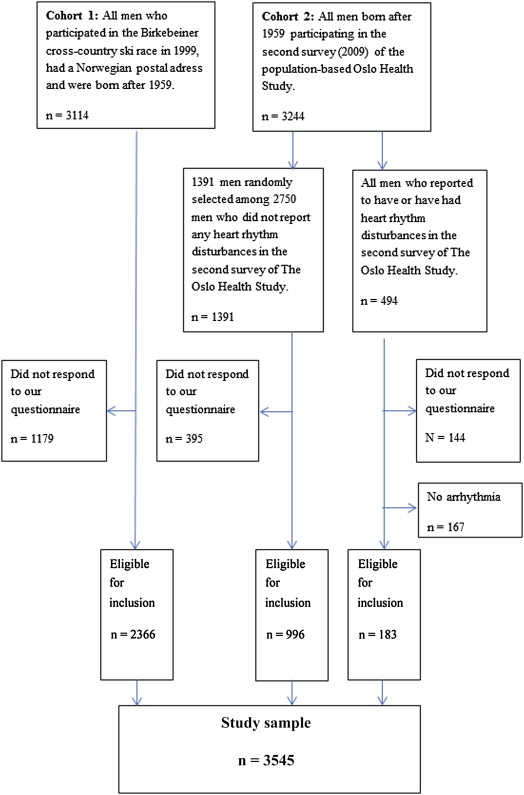
The first cohort comprised men who had previously participated in the 54-km Birkebeiner cross-country ski race. The cohort was constructed from a list provided by the race organizer. An invitation to take part in the study was sent to all 3,114 men who had participated in the race in 1999, were ≥40 years of age at that time, and had Norwegian postal addresses. The Birkebeiner race takes place in Norway annually and is among the most challenging cross-country ski races in the world. Cross-country skiing has been classified as a highly dynamic sport with moderate to high cardiovascular demand during competition, in the same category as running.
The second cohort included men examined as part of the population-based Oslo Health Study in 2000 to 2001 and 2009 who had given consent to be contacted for further studies. The participants of the study have been shown to represent the target population well. Of 2,750 men who did not report heart rhythm disturbances in the latter survey, 1,391 (51%) were randomly selected and invited to take part in the present study. In addition, all 494 men who had reported heart rhythm disturbances in the 2009 survey were invited to maximize the number of end points.
During 2012, all 4,999 invitees received an identical postal questionnaire ( Supplementary Data ) together with an information letter, and informed consent was obtained. The study was approved by the Regional Committee for Medical and Health Research Ethics and complied with the Declaration of Helsinki. Approvals for the review of the medical records were obtained from the responsible authorities for research and data protection for each hospital reported by ≥1 participant.
The main end points of the study were AF and atrial flutter validated by electrocardiograms. Medical records were reviewed by the first investigator according to a predefined protocol for subjects who reported AF in the questionnaire, stated a Norwegian public hospital as the place where AF had been diagnosed, and gave consent. Incident arrhythmias until December 31, 2012, were identified by electrocardiograms. In cases of uncertain diagnoses, an end point committee consisting of 2 experienced cardiologists was consulted. Lone AF and self-reported AF were secondary end points. AF was classified as “lone” if the review did not reveal other relevant diseases. In patients with hypertension, the arrhythmia was classified as lone AF if electrocardiogram findings were available and normal. Self-reported AF was a positive response to the question “Do you believe yourself that you have or have had atrial fibrillation?” The questionnaire also contained questions regarding type, frequency, and duration of the arrhythmia. Atrial flutter and other types of supraventricular tachycardia were not assessed in the questionnaire but were registered during the review of medical records.
The main exposure, cumulative years of regular endurance exercise, was defined in the questionnaire as regular endurance exercise for ≥30 minutes ≥3 times a week with the purpose of increasing physical endurance capacity and reported on an 8-level ordinal scale (“never,” “<5 years,” “5 to 9 years,” “10 to 19 years,” etc.). The scale was condensed from 8 to 5 categories with a cutoff at 40 years of training. Leisure time PA during the previous 12 months was reported on a scale previously used in middle-aged and old Swedish athletes and validated in a sample from the Norwegian population.
All covariates were assessed by questionnaires. Concomitant heart diseases (coronary heart disease, cardiac valve pathology, heart surgery) were condensed into the variable “heart disease.” A direct acyclic graph ( Supplementary Figure S1 ) and research review were used to identify covariates appropriate for adjustment; age, height, heart disease, hypertension, and diabetes were included in the model as established risk factors for AF. Affiliation with the Birkebeiner cohort and frequency of high-intensity exercise during the previous 12 months were included because they changed the effect estimates by ≥10%. Other possible confounding factors were tested but changed the effect estimates by <10%: marital status, education, body mass index, hypercholesterolemia, hyperthyroidism, tobacco use, frequency of alcohol consumption, binge drinking, familial AF, leisure time PA during the previous 12 months, and number of completed Birkebeiner races.
We used Student’s t test for means of continuous variables and Pearson’s chi-square test of independence for categorical variables to compare characteristics of the study participants. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were calculated by weighted logistic regression, and different selection probabilities were adjusted for by using inverse probability weighting: study participants who were invited because they had previously participated in the Birkebeiner race or because they had previously reported arrhythmias in the Oslo Health Study were weighted by 1 (all eligible men were invited). Men who were randomly selected from participants in the Oslo Health Study were weighted by 2 (1,391 of 2,750 men were invited). Because of the different selection probability, we report the weighted prevalence for the participants in the Oslo Health Study. We report estimates for the 2 distinct cohorts separately and for the whole study sample. Sensitivity analyses were performed after the exclusion of men aged ≥75 years, men who had been diagnosed with arrhythmia before the age of 40 years, men invited because they had previously reported heart rhythm disturbances, and men with self-reported AF but unavailable medical records. Subjects with missing data (<2%) were left out of the analyses. All statistical analyses were conducted using SPSS version 20.0 (IBM, Armonk, New York) or Stata version 12.1 (StataCorp LP, College Station, Texas).
Results
In all, 3,712 of 4,999 invited men (74%) participated in the study, 76% of the skiers and 72% of the men from the Oslo Health Study. One hundred sixty-seven men who had reported arrhythmias in the Oslo Health Study but did not report AF in the present study were excluded, leaving 3,545 men eligible for the analyses. Table 1 describes characteristics of the study participants by years of endurance exercise. Men with histories of long-term regular exercise were younger, taller, had lower body mass indexes, had higher educational level, and had a lower prevalence of concomitant heart disease, hypertension, and diabetes mellitus than men who had never exercised regularly.
| Variables | Years of Regular Endurance Exercise | ||
|---|---|---|---|
| None N = 661 Mean (Median, Range) | <30 N = 1151 Mean (Median, Range) | ≥30 N = 1733 Mean (Median, Range) | |
| Age (years) | 69.8 (71, 53–91) | 63.0 (61, 53–90) | 66.3 (66, 53–92) |
| Height (cm) | 178 (179, 150–204) | 180 (180, 158–197) | 179 (180, 160–200) |
| Weight (kg) | 82.0 (80, 50–124) | 82.8 (82, 55–140) | 78.0 (77, 51–122) |
| Body mass index (kg/m²) | 25.7 (25.1, 17.3–44.5) | 25.5 (25.1, 18.0–42.6) | 24.2 (24.0, 14.4–36.5) |
| Years of education | 9.6 (8, 0–23) | 13.7 (14, 0–29) | 14.0 (15, 0–29) |
| % of 661 | % of 1151 | % of 1733 | |
| Birkebeiner skiers | 16.0% | 64.6% | 87.7% |
| Leisure-time physical activity previous 12 months | |||
| Sedate | 44.5% | 24.5% | 8.7% |
| High | 1.5% | 8.9% | 26.4% |
| Exercise intensity previous 12 months | |||
| Did not exercise | 93.8% | 3.8% | 1.9% |
| Overweight of low intensity | 2.9% | 42.3% | 39.5% |
| Equal parts of low and high | 2.4% | 39.4% | 47.9% |
| Overweight of high intensity | 0.9% | 14.4% | 10.7% |
| Atrial fibrillation in first degree relatives | 6.8% | 6.7% | 6.3% |
| Concomitant heart disease | 21.0% | 9.2% | 10.2% |
| Hypertension | 47.4% | 31.1% | 26.7% |
| Diabetes mellitus | 10.1% | 6.3% | 4.8% |
| Current or previous daily smoking | 54.2% | 49.0% | 29.6% |
| Frequency of alcohol consume | |||
| <once/4 weeks | 16.0% | 10.2% | 13.3% |
| > once/week | 46.8% | 43.9% | 41.9% |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


