Prematurity
The terms ectopic beat, extrasystole and premature contraction are, for practical purposes, synonymous. They refer to an impulse originating from the atria, AV junction (i.e. the AV node together with the bundle of His) or ventricles that arises prematurely in the cardiac cycle (Figures 2.1–2.3).
By definition, an ectopic beat must arise earlier in the cardiac cycle than the next normally timed beat would be expected. Thus the interval between the ectopic beat and the preceding beat, i.e. the coupling interval, is shorter than the cycle length of the main rhythm. If this fact is ignored, other beats with abnormal configurations such as escape beats (Chapter 3) and intermittent bundle branch block (Chapter 4) may be misinterpreted as ectopic beats.
The site of origin of an ectopic beat can be determined by careful examination of the ECG. A single rhythm strip may be inadequate. Scrutiny of simultaneous recordings of several ECG leads is often necessary to detect the diagnostic clues (Figures 2.4, 2.5).
Figure 2.1 The second, fourth, sixth and eighth complexes are atrial ectopic beats. The ectopic P waves are premature and differ in shape from those of sinus origin (the PR intervals of the atrial ectopic beats are prolonged).
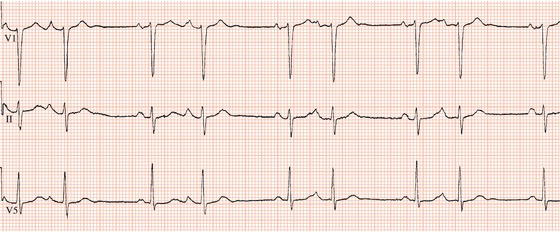
Figure 2.2 The fourth beat is a junctional ectopic beat (lead III). The junctional focus has activated the atria as well as the ventricles, resulting in an inverted P wave which precedes the QRS complex.


Figure 2.4 Simultaneous recording of leads V1 and V2. The third and sixth beats are unifocal ventricular ectopic beats. Their ventricular origin is not apparent in lead V1 but is obvious in V2.
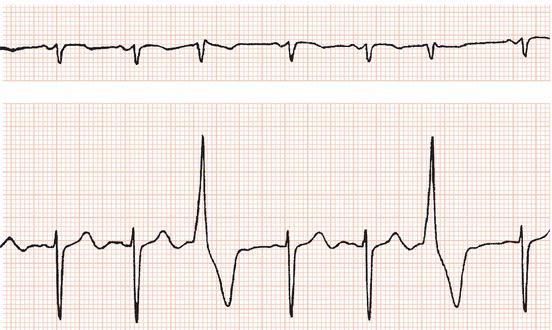
Figure 2.5 Atrial ectopic beats are superimposed on the T waves of the second, fourth and seventh ventricular complexes (lead V3). It can be seen how the T waves of these beats are modified by comparing them with the T wave of the first and sixth ventricular complexes, which are not followed by an atrial ectopic. The first two atrial ectopic beats are conducted with right bundle branch block.
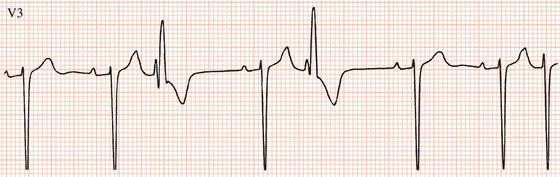
Figure 2.6 The last beat is an atrial ectopic beat conducted with a prolonged PR interval and right bundle branch block.

Atrial ectopic beats
P wave
An atrial ectopic beat results in a P wave that is premature. The site of origin and therefore direction of atrial activation will differ from that during sinus rhythm, so a premature P wave will usually differ in shape to a P wave of sinus node origin (Figure 2.1).
Because atrial ectopic beats are premature, they may be superimposed on and thus deform the T wave of the preceding beat. Careful examination of the ECG is essential to detect ectopic P waves; often, lead V1 is the best lead (Figures 2.5, 2.6).
Atrioventricular and intraventricular conduction
Usually the AV junction and bundle branches will conduct an atrial ectopic beat to the ventricles in the same manner as if the sinus node had activated the atria. Thus the PR interval and QRS complex of the ectopic beat will be identical to those during sinus rhythm (Figure 2.1). If the QRS complex during sinus rhythm is abnormal due to bundle branch block, then so will be the QRS complex of the ectopic beat.
Sometimes, however, atrial ectopic beats, especially those that arise very early in the cardiac cycle, may encounter either an AV junction or a bundle branch which has not yet recovered from conduction of the last atrial impulse and is, therefore, partially or completely refractory to excitation. Partial and complete refractoriness of the AV junction will result in prolongation of the PR interval and blocked atrial ectopic beats, respectively (Figures 2.1, 2.6–2.8). Atrial ectopics that are not conducted to the ventricles have been wrongly taken as an indication for cardiac pacing!
Partial or complete refractoriness of one or other bundle branch (it is usually the right bundle) will correspondingly lead to partial or complete bundle branch block (Figures 2.6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


