Carcinoid heart disease is a rare disease, and its prevalence is uncertain. The aim of the present prospective study was to assess the prevalence of carcinoid heart disease using annual echocardiographic follow-up. We studied 80 consecutive patients presenting with histologically proven digestive endocrine tumor and carcinoid syndrome. All patients underwent annual conventional transthoracic echocardiographic studies and measurement of biologic carcinoid markers. Right- and left-sided carcinoid heart disease and the score of the severity of carcinoid heart disease were systematically assessed. At baseline, the prevalence of right- and left-sided carcinoid heart disease was 33% and 8%, respectively. At the end of follow-up, the corresponding prevalence was 53% and 21%. The correlations were strong between urinary 5-hydroxyindoleacetic acid (5-HIAA) and the right-sided carcinoid heart disease score (r = 0.75, p <0.0001), between urinary 5-HIAA and the left-sided carcinoid heart disease score (r = 0.83, p = 0.001), and between urinary 5-HIAA and the overall carcinoid heart disease score (r = 0.84, p <0.0001). All patients with ≥3 years of carcinoid syndrome and increased level of urinary 5-HIAA presented with echocardiographic evidence of valve disease on routine monitoring. In conclusion, the prevalence of carcinoid heart disease remained high and increased during follow-up. Carcinoid heart disease progresses over time, highlighting the need for echocardiographic follow-up once carcinoid syndrome has been diagnosed.
Digestive endocrine tumor (carcinoid tumor) is a rare disease and can induce carcinoid heart disease in the case of carcinoid syndrome. However, <20% of digestive endocrine tumors induce carcinoid syndrome, owing to the release of vasoactive substances, especially serotonin. Carcinoid heart disease is mainly defined as valvular heart disease. The most frequent presentation of carcinoid heart disease is right-sided carcinoid heart disease, because of inactivation of serotonin by the lung. Left-sided carcinoid heart disease can also occur; however, reports have been uncommon. Most previous studies have been retrospective and were performed in the 1990s. Recently, improvement in the prognosis of patients with carcinoid heart disease has been reported. We hypothesized that the best management could modify the valvular characteristics of these patients. The aim of the present prospective study was to assess the prevalence of carcinoid heart disease in the modern therapeutic era.
Methods
From January 1998 to January 2007, we prospectively studied 80 consecutive patients referred to our institution for histologically proven digestive endocrine tumor and carcinoid syndrome. Carcinoid syndrome was defined as the presence of at least one of the following criteria: flushing, secretory diarrhea, or wheezing. The onset of the disease was defined as the beginning of the carcinoid symptoms. The metabolite of serotonin (urinary 5-hydroxyindoleacetic acid [5-HIAA]; normal value <40 mg/24 hours) and plasma chromogranin A (normal value <100 ng/ml) were assayed at baseline and during follow-up for all patients. Treatment was left to the discretion of the physician and was appropriate to the guidelines. Our institutional review board approved the study.
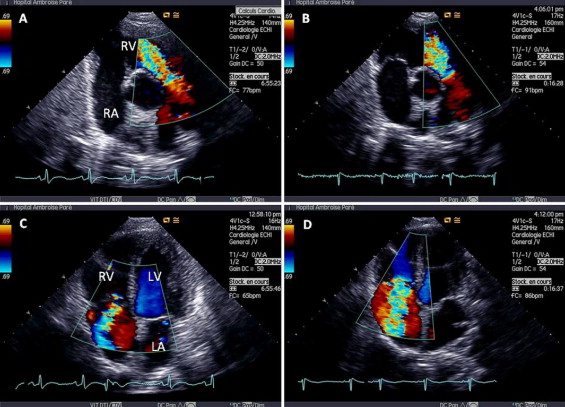
All patients underwent ≥2 transthoracic echocardiographic studies, with the same protocol, to detect and quantify valvular heart disease. During follow-up, each patient underwent annual echocardiographic examinations ( Figure 1 ). The readings were performed by the same investigator (NM), who was unaware of the clinical data. Carcinoid heart disease was strictly defined according to previously validated criteria. Right-sided carcinoid heart disease was defined as tricuspid or pulmonary valvular injury (i.e., thickening, retraction, reduced valvular mobility) associated with tricuspid regurgitation or stenosis or pulmonary regurgitation or stenosis. Right-sided carcinoid heart disease was quantified using a validated scoring system ( Table 1 ). The score for right-sided carcinoid heart disease was from 0 (no carcinoid heart disease) to 20 (major carcinoid heart disease). Left-sided carcinoid heart disease was defined as significant mitral or aortic regurgitation associated with a reduction in mitral or aortic valvular mobility. We also quantified left-sided carcinoid heart disease ( Table 1 ). The score for left-sided carcinoid heart disease was from 0 (no carcinoid heart disease) to 10 (major carcinoid heart disease). We thus obtained an overall score of carcinoid heart disease severity (ie, right- and left-sided carcinoid heart disease). This overall score was 0 to 30. Finally, the presence of myocardial metastases was systematically assessed.
| Carcinoid Heart Disease Scoring System | Score |
|---|---|
| Right-sided carcinoid heart disease (minimum score, 0; maximum, 20) | |
| Tricuspid and pulmonary anatomy (score for each valve) | |
| Normal | 0 |
| Mild immobility | 1 |
| Moderate to severe immobility | 2 |
| Thickened or fixed | 3 |
| Tricuspid and/or pulmonary regurgitation (score for each valve) | |
| No or trivial regurgitation | 0 |
| Mild regurgitation | 1 |
| Moderate regurgitation | 2 |
| Severe regurgitation | 3 |
| Tricuspid and/or pulmonary stenosis (score for each valve) | |
| No significant stenosis | 0 |
| Mild stenosis | 1 |
| Moderate stenosis | 2 |
| Severe stenosis | 3 |
| Right ventricular size | |
| Normal | 0 |
| Mild or moderate dilation | 1 |
| Severe dilation | 2 |
| Left-sided carcinoid heart disease scoring system (minimum score, 0; maximum, 10) | |
| Mitral and aortic anatomy (score for each valve) | |
| Normal | 0 |
| Mild immobility | 1 |
| Moderate to severe immobility | 2 |
| Thickened or fixed | 3 |
| Mitral and/or aortic regurgitation (score for each valve) | |
| No or mild regurgitation | 0 |
| Moderate regurgitation | 1 |
| Severe regurgitation | 2 |
The data were analyzed using StatView software, version 4.5 (SAS, Cary, North Carolina). Continuous variables are presented as the mean ± SD and qualitative variables as percentages. The continuous and categorical variables were compared using the chi-square test, unpaired t tests, and Fisher’s exact test, as appropriate. The prevalence of carcinoid heart disease was assessed at the first echocardiographic examination and at the end of follow-up. Linear regression analysis was used to investigate the relation between biologic markers and carcinoid heart disease. A value of p <0.05 indicated statistical significance.
Results
The baseline characteristics of our population are presented in Table 2 . No patient had a bronchial carcinoid tumor. Urinary 5-HIAA was significantly greater in patients with carcinoid heart disease (384 ± 431 mg/24 hours vs 43 ± 25 mg/24 hours in patients with carcinoid syndrome but without carcinoid heart disease; p <0.0001). Plasma chromogranin A was also significantly increased in patients with carcinoid heart disease (745 ± 1,097 ng/ml vs 86 ± 90 ng/ml in patients with carcinoid syndrome but without carcinoid heart disease; p <0.0001). Treatment is detailed in Table 2 . Surgical resection of the primary tumor was performed for all patients. Treatment was similar for the first 40 patients included compared to the final 40 patients included.
| Characteristic | Value |
|---|---|
| Age (years) | 62 ± 12 |
| Men | 38 (48%) |
| Primary tumor site | |
| Foregut | 8 (10%) |
| Stomach | 5 (6%) |
| Pancreas | 3 (4%) |
| Midgut | 64 (80%) |
| Ileojejunum | 60 (75%) |
| Proximal colon | 4 (5%) |
| Hindgut | 8 (10%) |
| Distal colon | 6 (8%) |
| Rectum | 2 (2%) |
| Metastases | 80 (100%) |
| Carcinoid syndrome symptoms | |
| Flushing | 63 (78%) |
| Secretory diarrhea | 49 (61%) |
| Wheezing | 17 (21%) |
| Treatment | |
| Somastatin analogue | 64 (80%) |
| Hepatic-artery embolization | 31 (39%) |
| Chemotherapy | 34 (43%) |
| Hepatic resection | 9 (11%) |
| Peak urinary 5-hydroxyindoleacetic acid level (mg/24 hours) | |
| Mean | 245 ± 347 |
| Range | 12–1,776 |
| Peak plasmatic chromogranin A (ng/ml) | |
| Mean | 449 ± 908 |
| Range | 22–5,777 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


