E
Emphysema
Emphysema is one of several diseases usually labeled collectively as chronic obstructive pulmonary disease. It’s the most common cause of death from respiratory disease in the United States. Emphysema appears to be more prevalent in men than in women; approximately 2 million Americans are affected with the disease. Postmortem findings reveal few adult lungs without some degree of emphysema.
CAUSES AND INCIDENCE
Emphysema may be caused by a genetic deficiency of alpha1-antitrypsin (AAT) and by cigarette smoking. Genetically, 1 in 3,000 newborns are found with the disease, and 1% to 3% of all cases of emphysema are due to AAT deficiency. Cigarette smoking is thought to cause up to 20% of the cases. Other causative factors are unknown.
Primary emphysema has been linked to an inherited deficiency of the enzyme AAT, a major component of alpha1-globulin. AAT inhibits the activation of several proteolytic enzymes; deficiency of this enzyme is an autosomal recessive trait that predisposes an individual to develop emphysema because proteolysis in lung tissues isn’t inhibited. Homozygous individuals have up to an 80% chance of developing lung disease; people who smoke have a greater chance of developing emphysema. Patients who develop emphysema before or during their early 40s and those who are nonsmokers are believed to have an AAT deficiency.
In emphysema, recurrent inflammation is associated with the release of proteolytic enzymes from lung cells. This causes irreversible enlargement of the air spaces distal to the terminal bronchioles. Enlargement of air spaces destroys the alveolar walls, which results in breakdown of elasticity and loss of fibrous and muscle tissue, thus making the lungs less compliant.
In normal breathing, the air moves into and out of the lungs to meet metabolic needs. A change in airway size compromises the lung’s ability to circulate sufficient air. In patient’s with emphysema, recurrent pulmonary inflammation damages and eventually destroys the alveolar walls, creating large air spaces. (See Air trapping in emphysema.)
The alveolar septa are initially destroyed, eliminating a portion of the capillary bed and increasing air volume in the acinus. This breakdown leaves the alveoli unable to recoil normally after expanding and
results in bronchiolar collapse on expiration. The damaged or destroyed alveolar walls can’t support the airways to keep them open.
results in bronchiolar collapse on expiration. The damaged or destroyed alveolar walls can’t support the airways to keep them open.
AIR TRAPPING IN EMPHYSEMA
After alveolar walls are damaged or destroyed, they can’t support the airways and keep them open. The alveolar walls then lose their elastic recoil capability. Collapse then occurs on expiration.
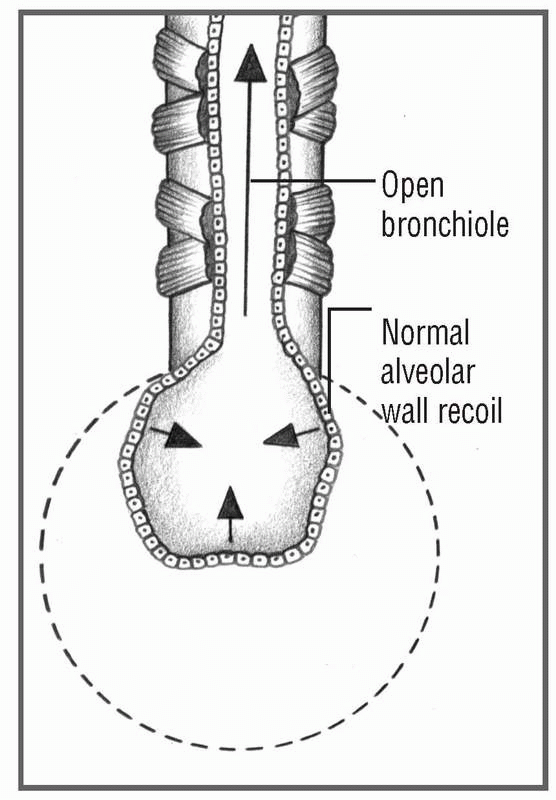
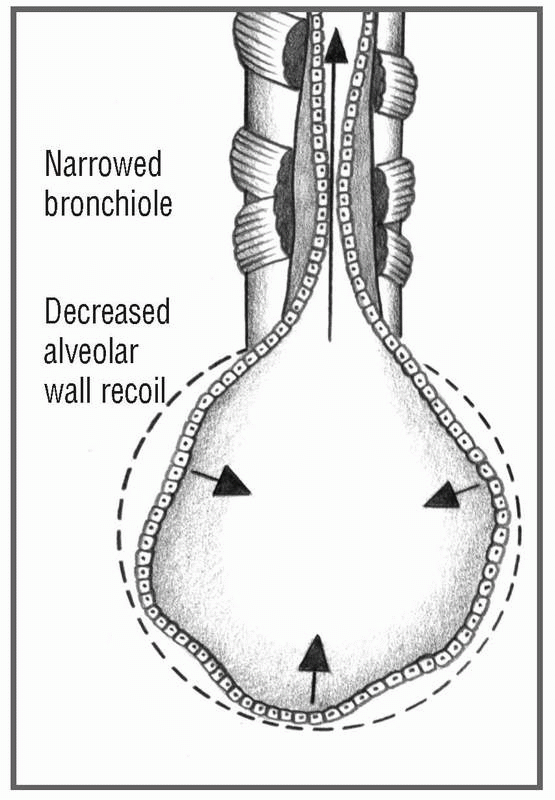
The amount of air that can be expired passively diminishes, thus trapping air in the lungs and leading to overdistention. Hyperinflation of the alveoli produces bullae (air spaces) adjacent to pleura (blebs). Septal destruction also decreases airway calibration. Part of each inspiration is trapped because of increased residual volume and decreased calibration. Septal destruction may affect only the respiratory bronchioles and alveolar ducts, leaving alveolar sacs intact, or it can involve the entire acinus with more random damage and involve the lower lobes of the lungs.
SIGNS AND SYMPTOMS
• By history, long-time smoker
• Shortness of breath
• Chronic cough
• Anorexia with resultant weight loss and a general feeling of malaise
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


