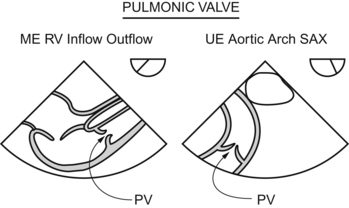
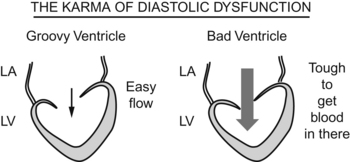
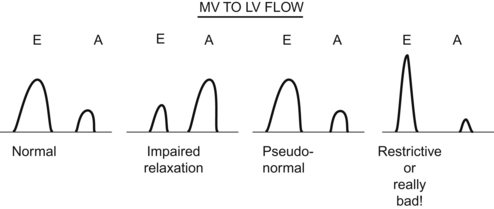
Chapter 8 Doppler Profiles and Assessment of Diastolic Function Christopher J. Gallagher and John C. Sciarra Also, if the hepatic vein flow profile shows systolic flow reversal, that also indicates severe tricuspid regurgitation. If you think about it, that makes sense. When the heart contracts, if the tricuspid valve doesn’t work, the blood flows back into the right atrium and just keeps on flowing backward, backward, backward, all the way back into the inferior vena cava and back further into the hepatic vein (which feeds into the inferior vena cava). Since the pulmonic valve lies far afield from the echo probe, getting more quantitative than that just ain’t in the works. The pump doesn’t work, but the concept of diastolic dysfunction is tough. The loading of the pump doesn’t work. The world would be a nice place if the mitral inflow patterns were a simple First, I’ll blast through the patterns, then I’ll go back and try to drag you through the reasoning. PLOW THROUGH THIS STUFF SLOWLY, AND LOOK FOR THE EXPLANATION IN A FEW DIFFERENT BOOKS, FOR DIASTOLIC DYSFUNCTION IS A TOUGHIE. Now, the reasoning behind the patterns. (The first part is easy—the second is a bit sticky.)
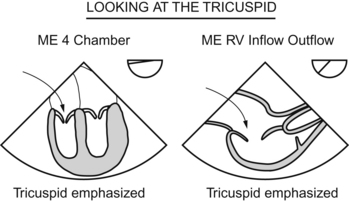
Tricuspid Valve and Right Ventricular Inflow
 The jet area is greater than 10 cm squared
The jet area is greater than 10 cm squared
 The jet area-to-right atrial area is greater than 67%
The jet area-to-right atrial area is greater than 67%
 The vena contracta width (narrowest width of the regurgitant jet) is >6.5 cm squared
The vena contracta width (narrowest width of the regurgitant jet) is >6.5 cm squared
 The tricuspid jet intensity is >65% of antegrade flow
The tricuspid jet intensity is >65% of antegrade flow
Pulmonary Valve and Right Ventricular Outflow
Mitral Valve and Left Ventricular Inflow

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


