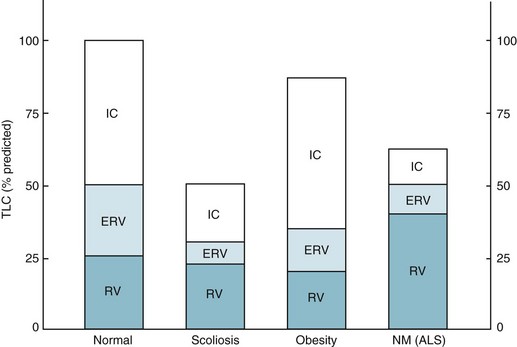
19 The major neuromuscular diseases that can affect the muscles of respiration are listed in Table 19-1; several are discussed here. Table 19-1 DISORDERS OF THE RESPIRATORY PUMP Impairment of inspiratory muscle strength may render patients unable to maintain sufficient minute ventilation for adequate CO2 elimination. In addition, patients often alter their pattern of breathing, taking shallower and more frequent breaths. Although this pattern of breathing may require less muscular effort and be more comfortable, it is also less efficient because a greater proportion of each breath is wasted on ventilating the anatomic dead space (see Chapter 1). Therefore, even if total minute ventilation is maintained, alveolar ventilation (and thus CO2 elimination) is impaired by the altered pattern of breathing. With severe neuromuscular disease, pulmonary function tests show a restrictive pattern of impairment. Although muscle weakness is the primary cause of restriction, compliance of the lung and chest wall may be secondarily affected, further contributing to the restrictive pattern. The decrease in pulmonary compliance presumably is due to microatelectasis (i.e., multiple areas of alveolar collapse) resulting from the shallow tidal volumes. At the same time, stiffening of various components of the chest wall (e.g., tendons, ligaments, and joints) over time is thought to be responsible for decreased distensibility of the chest wall. Functional residual capacity (FRC) is normal or decreased, depending on how much respiratory system compliance is altered. Total lung capacity is decreased primarily as a result of inspiratory muscle weakness, but changes in respiratory system compliance may contribute as well. Residual volume (RV) frequently is increased as a result of expiratory muscle weakness (Fig. 19-1). The degree of muscle weakness can be quantified by measuring the maximal inspiratory and expiratory pressures the patient is able to generate with maximal inspiratory and expiratory efforts against a closed mouthpiece. Both maximal inspiratory pressure (MIP) and maximal expiratory pressure may be significantly depressed. Inefficient diaphragmatic contraction is another factor that may contribute to diaphragmatic fatigue, especially in patients with obstructive lung disease. When the diaphragm is flattened and its fibers are shortened as a result of hyperinflated lungs, the force or pressure developed during contraction is less for any given level of diaphragmatic excitation (see Chapter 17). Therefore, a higher degree of stimulation is necessary to generate comparable pressure by the diaphragm, and increased energy consumption results.
Disorders of the Respiratory Pump
Neuromuscular Disease Affecting the Muscles of Respiration
Specific Diseases
Neuromuscular Diseases
Chest Wall Diseases
Guillain-Barré syndrome
Kyphoscoliosis
Myasthenia gravis
Obesity
Poliomyelitis
Ankylosing spondylitis
Postpolio syndrome
Amyotrophic lateral sclerosis
Cervical or thoracic spinal cord injury
Polymyositis
Muscular dystrophy
Pathophysiology and Clinical Consequences
Diaphragmatic Disease
Diaphragmatic Fatigue
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Disorders of the Respiratory Pump