Chapter 6 Diseases of the aorta
Introduction
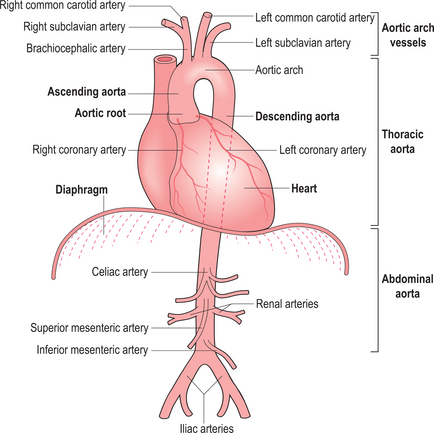
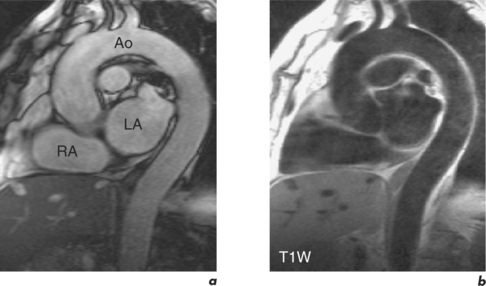
The aorta can be evaluated by a variety of techniques (Figure 6.1). X-ray contrast angiography was the gold standard method for many years but it is invasive and uses ionizing radiation and nephrotoxic contrast agents. Noninvasive options are TOE, CT and CMR (Figure 6.2). TOE is portable but relatively invasive and offers incomplete coverage of the aorta with restricted visualization at the aortic arch. CT is fast and widely available but uses ionizing radiation and nephrotoxic contrast agents. CMR avoids these limitations and offers multiplanar imaging of the aorta with a wide field of view and concurrent cardiac functional assessment. However, it is less available and evaluation of critically ill patients can be hampered by MRI-incompatible life support and monitoring equipment.
CMR reports of scans pertaining to the aorta follow the general pattern of:
Thoracic aortic aneurysm
An aortic aneurysm is a focal dilatation of the aorta. According to the shape the aneurysm is described as fusiform, with symmetrical dilatation of the circumference of the aorta, or saccular where only a part of the aortic wall is dilated. Aortic aneurysms can also be classified into true and false aneurysms. A true aneurysm consists of dilatation of all the layers of the aortic wall and characteristically has a wide neck. By contrast, in a false aneurysm perforation of the intima and media is contained by the surrounding adventitia and peri-aortic tissue, and the neck is usually narrow.
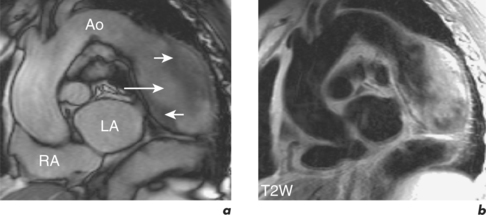
Aortic aneurysms are usually the consequence of atherosclerotic disease and most commonly occur at the descending aorta (Figure 6.3). Other causes are trauma, connective tissue disorders such as Marfan and Ehlers–Danlos syndromes, congenital abnormalities, and infections such as syphilis. Post-stenotic aneurysms are found distal to AV stenosis and aortic coarctation or recoarctation.
CMR can readily detect aortic aneurysms and scan protocols evaluate the following:
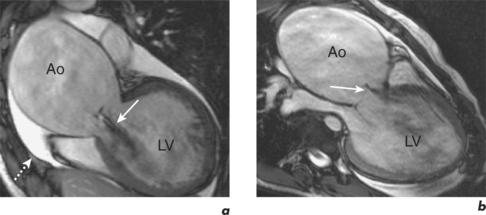
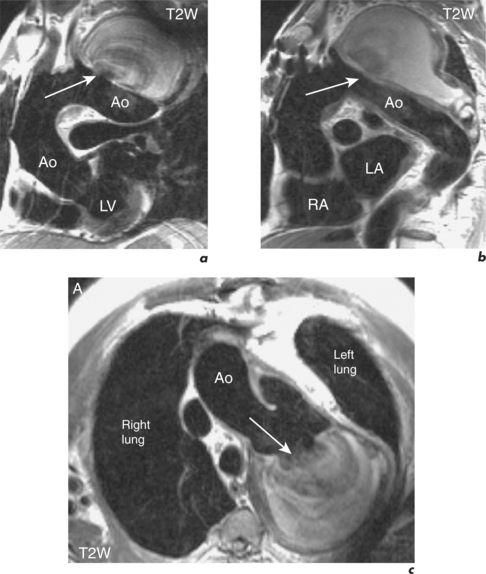
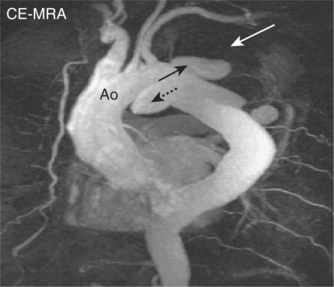
SE images acquired in the transverse and long-axis planes are useful for measuring the diameter of the aorta at different levels and relationship of the aneurysm to major vessels. Coronal and oblique sagittal views clearly depict the aortic root and tortuous segments. Slow or turbulent blood flow can produce images which mimic mural thrombus on SE imaging. SSFP cines and velocity flow mapping help to differentiate slow flow from intraluminal thrombus. Where intraluminal thrombus is present, its thickness and extent should be determined. CMR allows characterization of intraluminal thrombus based on signal changes caused by the paramagnetic properties of deoxyhaemoglobin and methaemoglobin. Methaemoglobin forms from red blood cell lysis and shortens T1 but increases T2, causing hyperintensity on both T1W and T2W SE sequences. Thrombus with homogeneous low signal intensity on both T1W and T2W images corresponds to macroscopic organized thrombus. Some organized thrombi may have an internal rim of hyperintensity which represents recent clot apposition on the luminal surface of the thrombus. Thrombi with homogeneous high signal intensity on T1W and T2W imaging represent unorganized thrombi, composed mainly of fresh clot. Some thrombi may appear partially organized, with areas of high and low signal intensity (Figure 6.5). Inflammatory aortic aneurysms may show an area of peri-aortic inflammation that enhances following gadolinium contrast. This can be better visualized using a T1W CMR sequence with an added fat saturation prepulse. MRA is useful for assessing aortic flow and involvement and patency of aortic branch vessels. Images are acquired in the aortic long-axis plane and can then be reformatted into the transaxial plane. Post-processing techniques, such as maximum intensity projections (MIPs) and shaded surface displays, are used for representation (Figure 6.6). CMR is useful for follow-up evaluation of aneurysm size and serial measurements must be made at the same level.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


